

Esophago-glottal closure reflex in human infants: a novel reflex elicited with concurrent manometry and ultrasonography
- PMID: 17617206
- PMCID: PMC4028634
- DOI: 10.1111/j.1572-0241.2007.01401.x
Esophago-glottal closure reflex in human infants: a novel reflex elicited with concurrent manometry and ultrasonography
Abstract
Background and aims: Our aims were to identify and characterize the glottal response to esophageal mechanostimulation in human infants. We tested the hypotheses that glottal response is related to the type of esophageal peristaltic response, stimulus volume, and respiratory phase.
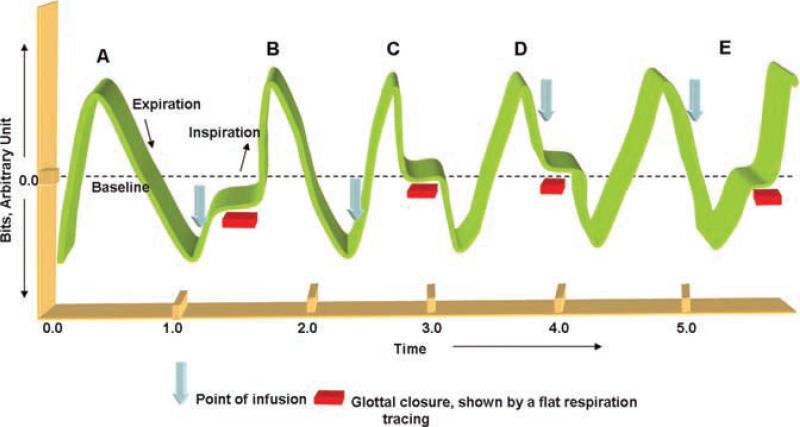
Methods: Ten infants (2.8 kg, SD 0.5) were studied at 39.2 wk (SD 2.4). Esophageal manometry concurrent with ultrasonography of the glottis (USG) was performed. The sensory-motor characteristics of mechanostimulation-induced esophago-glottal closure reflex (EGCR, adduction of glottal folds upon esophageal provocation) were identified. Mid-esophageal infusions of air (N = 41) were given and the temporal relationships of glottal response with deglutition, secondary peristalsis (SP), and the respiratory phase were analyzed using multinomial logistic regression models.
Results: The frequency occurrence of EGCR (83%) was compared (P < 0.001) with deglutition (44%), SP (34%), and no esophageal responses (22%). The odds ratios (OR, 95% CI) for the coexistence of EGCR with SP (0.4, 0.06-2.2), deglutition (1.9, 0.1-26), and no response (1.9, 0.4-9.0) were similar. The response time for esophageal reflexes was 3.8 (SD 1.8) s, and for EGCR was 0.4 (SD 0.3) s (P < 0.001). Volume-response relationship was noted (1 mL vs 2 mL, P < 0.05). EGCR was noted in both respiratory phases; however, EGCR response time was faster during expiration (P < 0.05).
Conclusion: The occurrence of EGCR is independent of the peristaltic reflexes or the respiratory phase of infusion. The independent existence of EGCR suggests a hypervigilant state of the glottis to prevent retrograde aspiration during GER events.
Figures



Similar articles
-
Definition and implications of novel pharyngo-glottal reflex in human infants using concurrent manometry ultrasonography.Am J Gastroenterol. 2009 Oct;104(10):2572-82. doi: 10.1038/ajg.2009.411. Epub 2009 Jul 14. Am J Gastroenterol. 2009. PMID: 19603008 Free PMC article.
-
Mechanisms of reflexes induced by esophageal distension.Am J Physiol Gastrointest Liver Physiol. 2001 Nov;281(5):G1246-63. doi: 10.1152/ajpgi.2001.281.5.G1246. Am J Physiol Gastrointest Liver Physiol. 2001. PMID: 11668034
-
Esophageal sensation in premature human neonates: temporal relationships and implications of aerodigestive reflexes and electrocortical arousals.Am J Physiol Gastrointest Liver Physiol. 2012 Jan 1;302(1):G134-44. doi: 10.1152/ajpgi.00067.2011. Epub 2011 Aug 18. Am J Physiol Gastrointest Liver Physiol. 2012. PMID: 21852361 Free PMC article.
-
Reflex-mediated enhancement of airway protective mechanisms.Am J Med. 2000 Mar 6;108 Suppl 4a:8S-14S. doi: 10.1016/s0002-9343(99)00289-2. Am J Med. 2000. PMID: 10718445 Review.
-
Central integration of swallow and airway-protective reflexes.Am J Med. 2000 Mar 6;108 Suppl 4a:62S-67S. doi: 10.1016/s0002-9343(99)00340-x. Am J Med. 2000. PMID: 10718454 Review.
Cited by
-
Ultrasound imaging of infant swallowing during breast-feeding.Dysphagia. 2010 Sep;25(3):183-91. doi: 10.1007/s00455-009-9241-0. Epub 2009 Jul 22. Dysphagia. 2010. PMID: 19626366
-
Current perspectives on reflux laryngitis.Clin J Gastroenterol. 2014 Dec;7(6):471-5. doi: 10.1007/s12328-014-0535-x. Epub 2014 Nov 1. Clin J Gastroenterol. 2014. PMID: 25491904 Review.
-
Maturation Modulates Pharyngeal-Stimulus Provoked Pharyngeal and Respiratory Rhythms in Human Infants.Dysphagia. 2018 Feb;33(1):63-75. doi: 10.1007/s00455-017-9833-z. Epub 2017 Aug 21. Dysphagia. 2018. PMID: 28828751 Free PMC article.
-
Characterization of Esophageal and Sphincter Reflexes across Maturation in Dysphagic Infants with Oral Feeding Success vs Infants requiring Gastrostomy.Dysphagia. 2022 Feb;37(1):148-157. doi: 10.1007/s00455-021-10258-8. Epub 2021 Feb 12. Dysphagia. 2022. PMID: 33576892
-
Pharyngoesophageal motility reflex mechanisms in the human neonate: importance of integrative cross-systems physiology.Am J Physiol Gastrointest Liver Physiol. 2021 Aug 1;321(2):G139-G148. doi: 10.1152/ajpgi.00480.2020. Epub 2021 Jun 9. Am J Physiol Gastrointest Liver Physiol. 2021. PMID: 34105355 Free PMC article. Review.
References
-
- Jadcherla SR, Rudolph CD. Gastroesophageal reflux in the preterm neonate. Neo Reviews. 2005;6:e87–98.
-
- Orenstein SR. An overview of reflux-associated disorders in infants: Apnea, laryngospasm, and aspiration. Am J Med. 2001;111:60S–3S. - PubMed
-
- Nelson SP, Chen EH, Syniar GM, et al. Prevalence of symptoms of gastroesophageal reflux during infancy. A pediatric practice-based survey. Pediatric Practice Research Group. Arch Pediatr Adolesc Med. 1997;151:569–72. - PubMed
-
- Shaker R, Hogan WJ. Reflex-mediated enhancement of airway protective mechanisms. Am J Med. 2000;108(Suppl 4a):8S–14S. - PubMed
-
- Shaker R, Dodds WJ, Ren J, et al. Esophagoglottal closure reflex: A mechanism of airway protection. Gastroenterology. 1992;102:857–61. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
