

Variations in corticosteroid/anesthetic injections for painful shoulder conditions: comparisons among orthopaedic surgeons, rheumatologists, and physical medicine and primary-care physicians
- PMID: 17617900
- PMCID: PMC1950874
- DOI: 10.1186/1471-2474-8-63
Variations in corticosteroid/anesthetic injections for painful shoulder conditions: comparisons among orthopaedic surgeons, rheumatologists, and physical medicine and primary-care physicians
Abstract
Background: Variations in corticosteroid/anesthetic doses for injecting shoulder conditions were examined among orthopaedic surgeons, rheumatologists, and primary-care sports medicine (PCSMs) and physical medicine and rehabilitation (PMRs) physicians to provide data needed for documenting inter-group differences for establishing uniform injection guidelines.
Methods: 264 surveys, sent to these physicians in our tri-state area of the western United States, addressed corticosteroid/anesthetic doses and types used for subacromial impingement, degenerative glenohumeral and acromioclavicular arthritis, biceps tendinitis, and peri-scapular trigger points. They were asked about preferences regarding: 1) fluorinated vs. non-fluorinated corticosteroids, 2) acetate vs. phosphate types, 3) patient age, and 4) adjustments for special considerations including young athletes and diabetics.
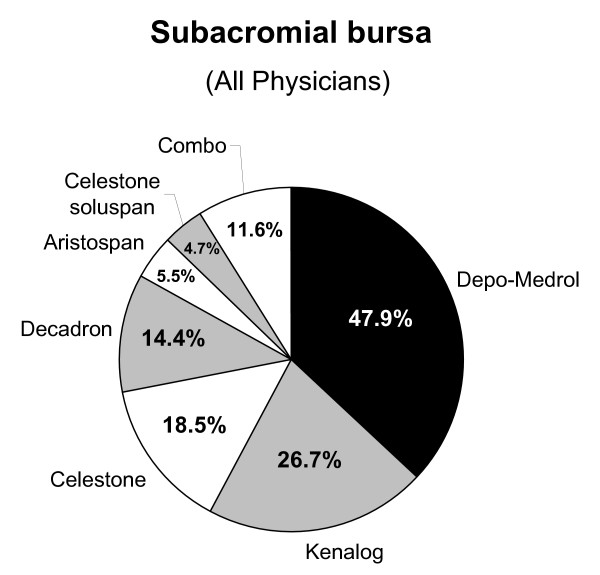
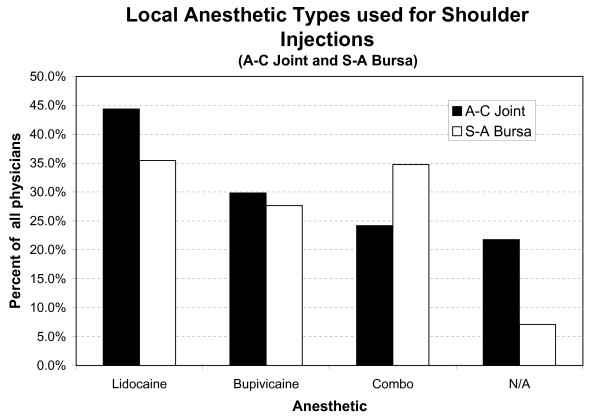
Results: 169 (64% response rate, RR) surveys were returned: 105/163 orthopaedic surgeons (64%RR), 44/77 PCSMs/PMRs (57%RR), 20/24 rheumatologists (83%RR). Although corticosteroid doses do not differ significantly between specialties (p > 0.3), anesthetic volumes show broad variations, with surgeons using larger volumes. Although 29% of PCSMs/PMRs, 44% rheumatologists, and 41% surgeons exceed "recommended" doses for the acromioclavicular joint, >98% were within recommendations for the subacromial bursa and glenohumeral joint. Depo-Medrol(R) (methylprednisolone acetate) and Kenalog(R) (triamcinolone acetonide) are most commonly used. More rheumatologists (80%) were aware that there are acetate and phosphate types of corticosteroids as compared to PCSMs/PMRs (76%) and orthopaedists (60%). However, relatively fewer rheumatologists (25%) than PCSMs/PMRs (32%) or orthopaedists (32%) knew that phosphate types are more soluble. Fluorinated corticosteroids, which can be deleterious to soft tissues, were used with these frequencies for the biceps sheath: 17% rheumatologists, 8% PCSMs/PMRs, 37% orthopaedists. Nearly 85% use the same non-fluorinated corticosteroid for all injections; <10% make adjustments for diabetic patients.
Conclusion: Variations between specialists in anesthetic doses suggest that surgeons (who use significantly larger volumes) emphasize determining the percentage of pain attributable to the injected region. Alternatively, this might reflect a more profound knowledge that non-surgeons specialists have of the potentially adverse cardiovascular effects of these agents. Variations between these specialists in corticosteroid/anesthetic doses and/or types, and their use in some special situations (e.g., diabetics), bespeak the need for additional investigations aimed at establishing uniform injection guidelines, and for identifying knowledge deficiencies that warrant advanced education.
Figures
Similar articles
-
Orthopaedists' and family practitioners' knowledge of simple low back pain management.Spine (Phila Pa 1976). 2009 Jul 1;34(15):1600-3. doi: 10.1097/BRS.0b013e3181a96622. Spine (Phila Pa 1976). 2009. PMID: 19564770
-
Analysis of pharmacologic and nonpharmacologic prescription patterns of general practitioners and specialists in the AMICA study.Semin Arthritis Rheum. 2005 Aug;35(1 Suppl 1):24-30. doi: 10.1016/j.semarthrit.2005.02.001. Semin Arthritis Rheum. 2005. PMID: 16084230
-
Subacromial triamcinolone acetonide, hyaluronic acid and saline injections for shoulder pain an RCT investigating the effectiveness in the first days.BMC Musculoskelet Disord. 2014 Oct 23;15:352. doi: 10.1186/1471-2474-15-352. BMC Musculoskelet Disord. 2014. PMID: 25341673 Free PMC article. Clinical Trial.
-
Corticosteroid injection therapy for overuse injuries.Am Fam Physician. 1995 Nov 1;52(6):1811-6. Am Fam Physician. 1995. PMID: 7484691 Review.
-
Corticosteroid injections for painful shoulders.Int J Clin Pract. 2005 Oct;59(10):1178-86. doi: 10.1111/j.1368-5031.2005.00640.x. Int J Clin Pract. 2005. PMID: 16178986 Review.
Cited by
-
The SAInT study: a protocol for a randomized controlled trial of steroid injection for subacromial pain syndrome using the anterolateral versus posterior approach.Bone Jt Open. 2024 Sep 3;5(9):729-735. doi: 10.1302/2633-1462.59.BJO-2023-0138.R1. Bone Jt Open. 2024. PMID: 39223986 Free PMC article.
-
Value of MR arthrography findings for pain relief after glenohumeral corticosteroid injections in the short term.Eur Radiol. 2019 Dec;29(12):6416-6424. doi: 10.1007/s00330-019-06237-1. Epub 2019 Jun 17. Eur Radiol. 2019. PMID: 31209618
-
Ultrasound guided injection of dexamethasone versus placebo for treatment of plantar fasciitis: protocol for a randomised controlled trial.J Foot Ankle Res. 2010 Jul 16;3:15. doi: 10.1186/1757-1146-3-15. J Foot Ankle Res. 2010. PMID: 20633300 Free PMC article.
-
Corticosteroid injections compared to foot orthoses for plantar heel pain: protocol for the SOOTHE heel pain randomised trial.Contemp Clin Trials Commun. 2016 Nov 23;5:1-11. doi: 10.1016/j.conctc.2016.11.003. eCollection 2017 Mar. Contemp Clin Trials Commun. 2016. PMID: 29740617 Free PMC article.
-
Corticosteroid and Local Anesthetic Use Trends for Large Joint and Bursa Injections: Results of a Survey of Sports Medicine Physicians.PM R. 2021 Sep;13(9):962-968. doi: 10.1002/pmrj.12499. Epub 2020 Nov 23. PM R. 2021. PMID: 32969178 Free PMC article.
References
-
- Wise C. Arthrocentesis and Injection of Joints and Soft Tissues. In: Harris ED, Bud RC, Genovese MC, Firestein GS, Ruddy S, editor. Kelley's Textbook of Rheumatology. Vol. 1. Philadelphia: W.B. Saunders; 2005. pp. 692–709.
-
- Noerdlinger MA, Fadale PD. The role of injectable corticosteroids in orthopedics. Orthopedics. 2001;24:400–405. - PubMed
-
- Tallia AF, Cardone DA. Diagnostic and therapeutic injection of the shoulder region. Am Fam Physician. 2003;67:1271–1278. - PubMed
-
- Saunders S. Injection techniques in orthopaedic and sports medicine. 2. London: W.B. Saunders; 2002.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
