

Gabapentin and postoperative pain: a qualitative and quantitative systematic review, with focus on procedure
- PMID: 17617920
- PMCID: PMC1950698
- DOI: 10.1186/1471-2253-7-6
Gabapentin and postoperative pain: a qualitative and quantitative systematic review, with focus on procedure
Abstract
Background: Gabapentin is an antiepileptic drug used in a variety of chronic pain conditions. Increasing numbers of randomized trials indicate that gabapentin is effective as a postoperative analgesic. This procedure-specific systematic review aims to analyse the 24-hour postoperative effect of gabapentin on acute pain in adults.
Methods: Medline, The Cochrane Library and Google Scholar were searched for double-blind randomized placebo controlled trials of gabapentin for postoperative pain relief compared with placebo, in adults undergoing a surgical procedure. Qualitative analysis of postoperative effectiveness was evaluated by assessment of significant difference (P < 0.05) in pain relief using consumption of supplemental analgesic and pain scores between study groups. Quantitative analyses of combined data from similar procedures, were performed by calculating the weighted mean difference (WMD) of 24-hour cumulated opioid requirements, and the WMD for visual analogue scale (VAS) pain, (early (6 h) and late (24 h) postoperatively), between study groups. Side-effects (nausea, vomiting, dizziness and sedation) were extracted for calculation of their relative risk (RR).
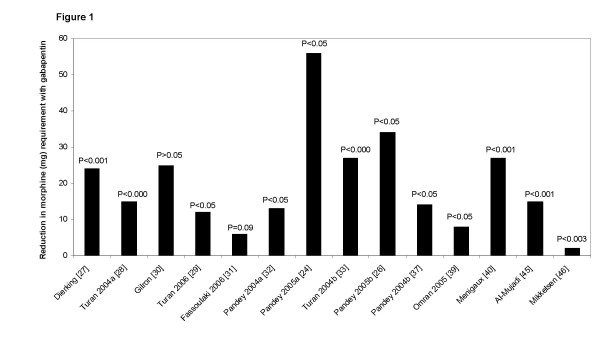
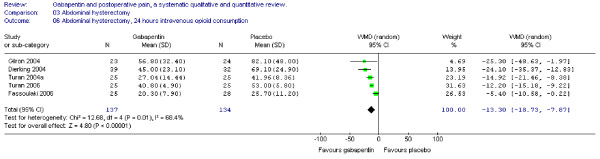
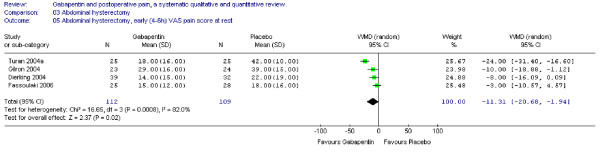
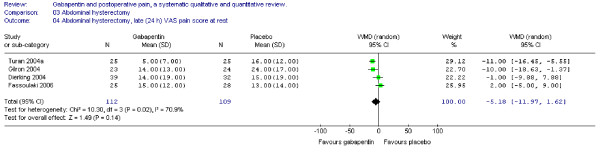
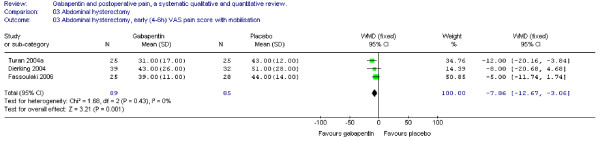
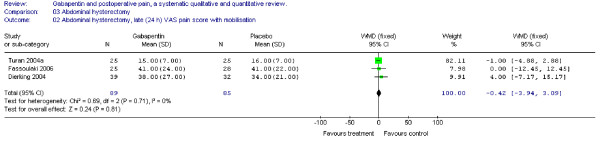
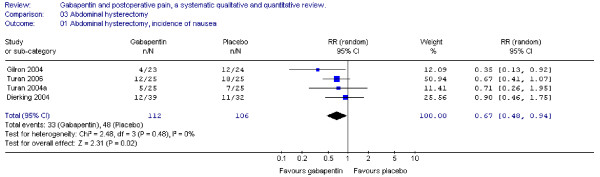
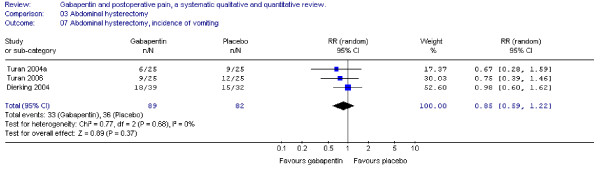
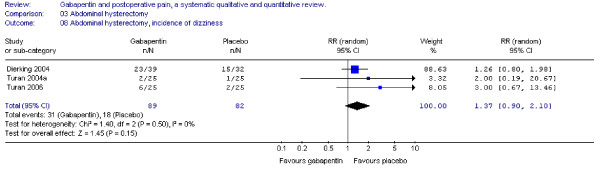
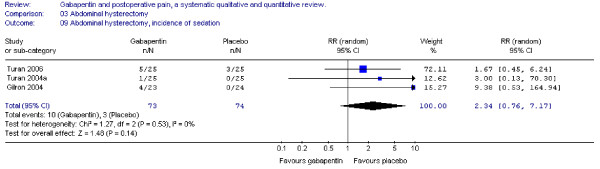
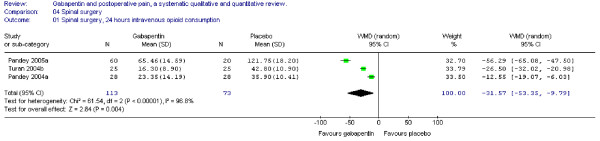
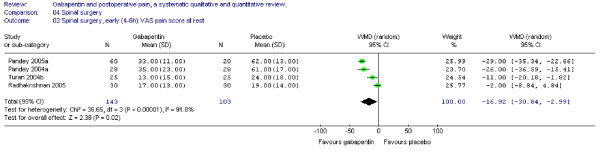
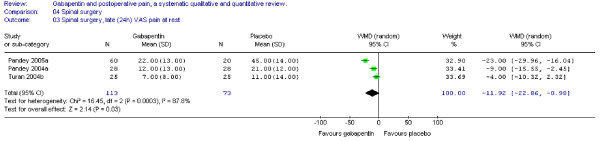
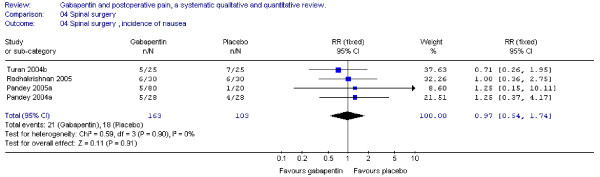
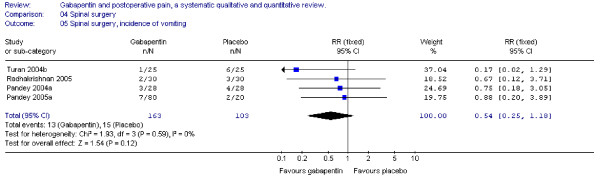
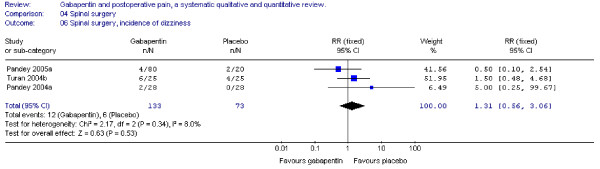
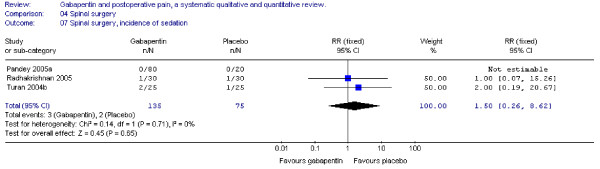
Results: Twenty-three trials with 1529 patients were included. In 12 of 16 studies with data on postoperative opioid requirement, the reported 24-hour opioid consumption was significantly reduced with gabapentin. Quantitative analysis of five trials in abdominal hysterectomy showed a significant reduction in morphine consumption (WMD - 13 mg, 95% confidence interval (CI) -19 to -8 mg), and in early pain scores at rest (WMD - 11 mm on the VAS, 95% CI -12 to -2 mm) and during activity (WMD -8 mm on the VAS; 95% CI -13 to -3 mm), favouring gabapentin. In spinal surgery, (4 trials), analyses demonstrated a significant reduction in morphine consumption (WMD of - 31 mg (95%CI - 53 to -10 mg) and pain scores, early (WMD - 17 mm on the VAS; 95 % CI -31 to -3 mm) and late (WMD -12 mm on the VAS; 95% CI -23 to -1 mm) also favouring gabapentin treatment. Nausea was improved with gabapentin in abdominal hysterectomy (RR 0.7; 95 % CI 0.5 to 0.9). Other side-effects were unaffected.
Conclusion: Perioperative use of gabapentin has a significant 24-hour opioid sparing effect and improves pain score for both abdominal hysterectomy and spinal surgery. Nausea may be reduced in abdominal hysterectomy.
Figures
References
LinkOut - more resources
Full Text Sources
Medical
