

Effect sizes of non-surgical treatments of non-specific low-back pain
- PMID: 17619914
- PMCID: PMC2223333
- DOI: 10.1007/s00586-007-0379-x
Effect sizes of non-surgical treatments of non-specific low-back pain
Abstract
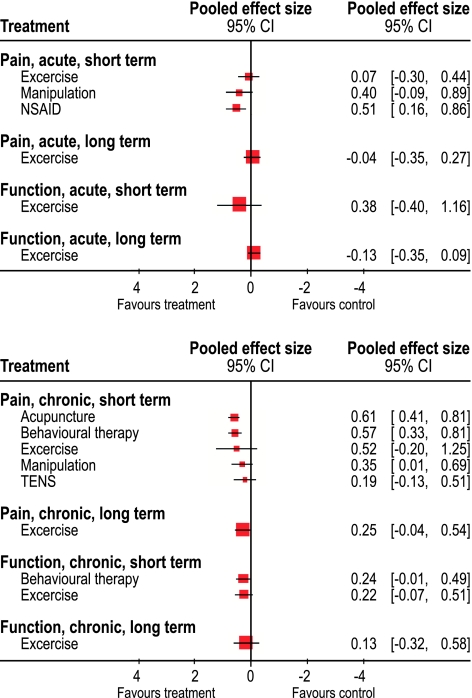
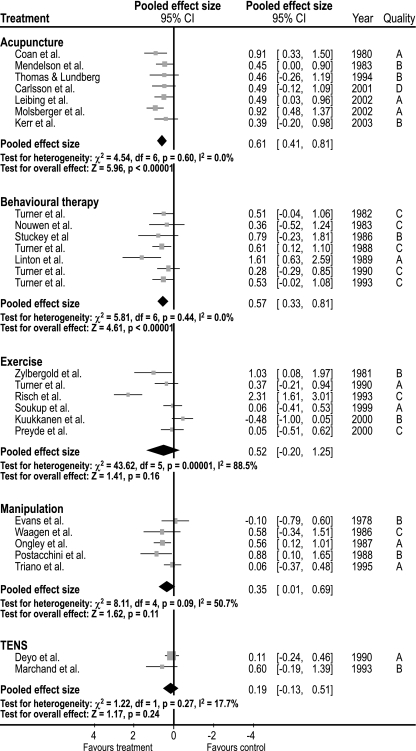
Numerous randomized trials have been published investigating the effectiveness of treatments for non-specific low-back pain (LBP) either by trials comparing interventions with a no-treatment group or comparing different interventions. In trials comparing two interventions, often no differences are found and it raises questions about the basic benefit of each treatment. To estimate the effect sizes of treatments for non-specific LBP compared to no-treatment comparison groups, we searched for randomized controlled trials from systematic reviews of treatment of non-specific LBP in the latest issue of the Cochrane Library, issue 2, 2005 and available databases until December 2005. Extracted data were effect sizes estimated as Standardized Mean Differences (SMD) and Relative Risk (RR) or data enabling calculation of effect sizes. For acute LBP, the effect size of non-steroidal anti-inflammatory drugs (NSAIDs) and manipulation were only modest (ES: 0.51 and 0.40, respectively) and there was no effect of exercise (ES: 0.07). For chronic LBP, acupuncture, behavioral therapy, exercise therapy, and NSAIDs had the largest effect sizes (SMD: 0.61, 0.57, and 0.52, and RR: 0.61, respectively), all with only a modest effect. Transcutaneous electric nerve stimulation and manipulation had small effect sizes (SMD: 0.22 and 0.35, respectively). As a conclusion, the effect of treatments for LBP is only small to moderate. Therefore, there is a dire need for developing more effective interventions.
Figures
References
-
- Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, Mannion AF, Reis S, Staal JB, Ursin H, Zanoli G. Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006;15(Suppl 2):S192–S300. doi: 10.1007/s00586-006-1072-1. - DOI - PMC - PubMed
-
- Arbus L, Fajadet B, Aubert D, Morre M, Goldfinger E. Activity of tetrazepam in low back pain. Clin Trials J. 1990;27:58–67.
-
- Assendelft WJ, Morton SC, Yu EI, Suttorp MJ, Shekelle PG (2004) Spinal manipulative therapy for low back pain. Cochrane Database Syst Rev CD000447 - PubMed
-
- Aure OF, Nilsen JH, Vasseljen O (2003) Manual therapy and exercise therapy in patients with chronic low back pain: a randomized, controlled trial with 1-year follow-up. Spine 28:525–531; discussion 531–522 - PubMed
-
- Babej-Dolle R, Freytag S, Eckmeyer J, Zerle G, Schinzel S, Schmeider G, Stankov G. Parenteral dipyrone versus diclofenac and placebo in patients with acute lumbago or sciatic pain: randomized observer-blind multicenter study. Int J Clin Pharmacol Ther. 1994;32:204–209. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
