

The efficacy and safety of drug treatments for chronic insomnia in adults: a meta-analysis of RCTs
- PMID: 17619935
- PMCID: PMC2219774
- DOI: 10.1007/s11606-007-0251-z
The efficacy and safety of drug treatments for chronic insomnia in adults: a meta-analysis of RCTs
Abstract
Background: Hypnotics have a role in the management of acute insomnia; however, the efficacy and safety of pharmacological interventions in the management of chronic insomnia is unclear.
Objective: The objective of this paper is to conduct a systematic review of the efficacy and safety of drug treatments for chronic insomnia in adults.
Data sources: Twenty-one electronic databases were searched, up to July 2006.
Study selection: Randomized double-blind, placebo-controlled trials were eligible. Quality was assessed using the Jadad scale. Data were pooled using the random effects model.
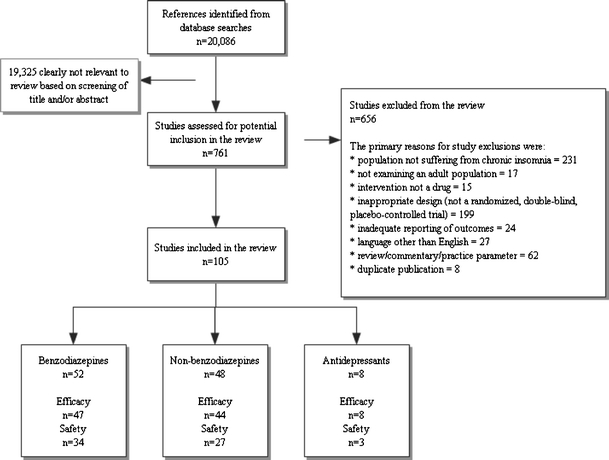
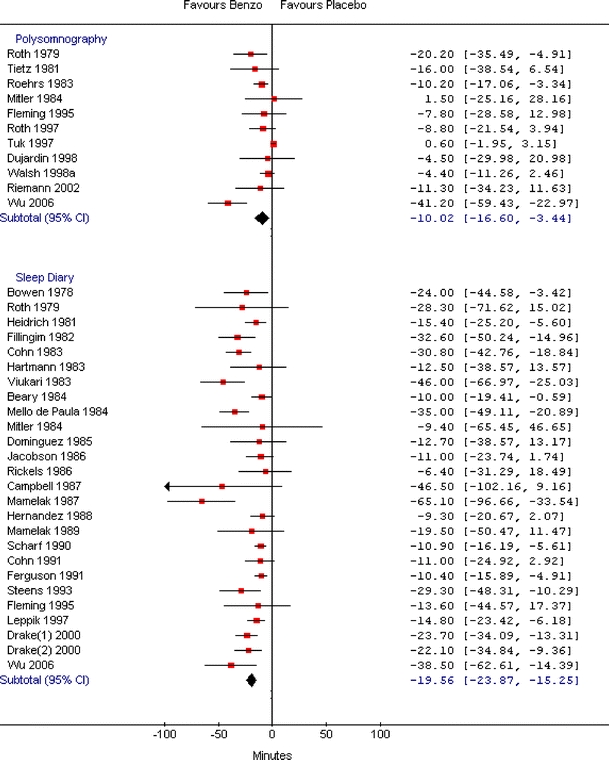
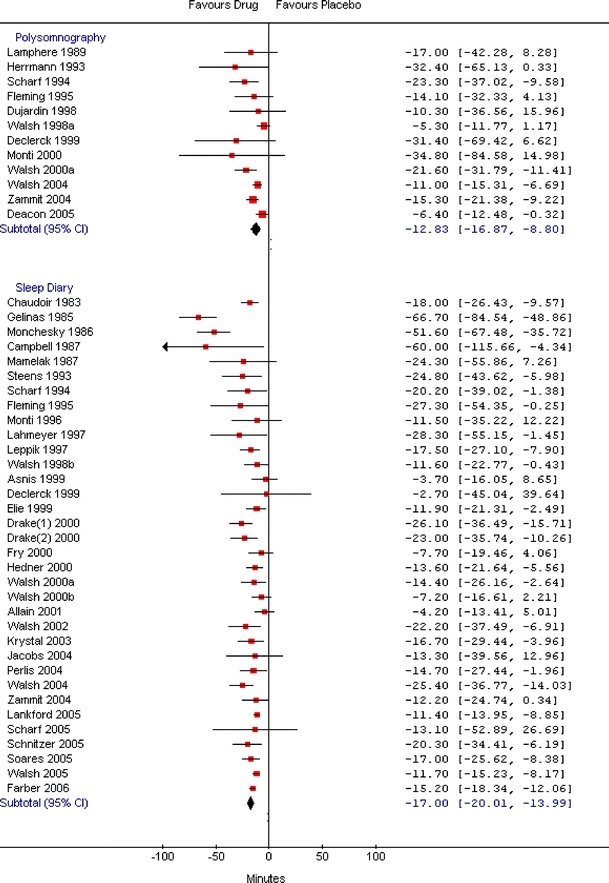
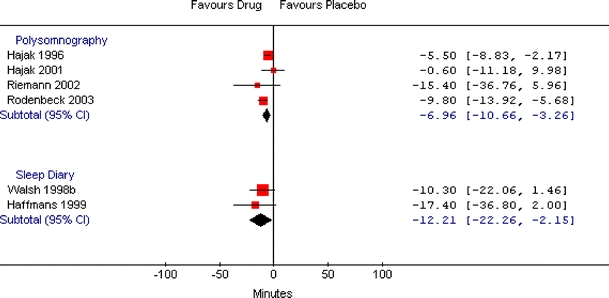
Data synthesis: One hundred and five studies were included in the review. Sleep onset latency, as measured by polysomnography, was significantly decreased for benzodiazepines (BDZ), (weighted mean difference: -10.0 minutes; 95% CI: -16.6, -3.4), non-benzodiazepines (non-BDZ) (-12.8 minutes; 95% CI: -16.9, -8.8) and antidepressants (ADP) (-7.0 minutes; 95% CI: -10.7, -3.3). Sleep onset latency assessed by sleep diaries was also improved (BDZ: -19.6 minutes; 95% CI: -23.9, -15.3; non-BDZ: -17.0 minutes; 95% CI: -20.0, -14.0; ADP: -12.2 minutes; 95% CI: -22.3, -2.2). Indirect comparisons between drug categories suggest BDZ and non-BDZ have a similar effect. All drug groups had a statistically significant higher risk of harm compared to placebo (BDZ: risk difference [RD]: 0.15; non-BDZ RD: 0.07; and ADP RD: 0.09), although the most commonly reported adverse events were minor. Indirect comparisons suggest that non-BDZ are safer than BDZ.
Conclusions: Benzodiazepines and non-benzodiazepines are effective treatments in the management of chronic insomnia, although they pose a risk of harm. There is also some evidence that antidepressants are effective and that they pose a risk of harm.
Figures
References
-
- Sateia MJ, Doghramji K, Hauri P, Morin CM. Evaluation of chronic insomnia. An American Academy of Sleep Medicine Review. Sleep 2000;23:1–66. - PubMed
-
- Simon GE, VonKorff M. Prevalence, burden, and treatment of insomnia in primary care. Am J Psychiatry. 1997;54:1417–23. - PubMed
-
- Leger D, Guilleminault C, Bader G, Levy E, Paillard M. Medical and socio-professional impact of insomnia. Sleep 2002;25:625–9. - PubMed
-
- Ohayon M. Epidemiological study on insomnia in the general population. Sleep 1996;19(3 suppl):S7–15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
