

Clinical impact and cost-effectiveness of antiretroviral therapy in India: starting criteria and second-line therapy
- PMID: 17620747
- PMCID: PMC2365748
- DOI: 10.1097/01.aids.0000279714.60935.a2
Clinical impact and cost-effectiveness of antiretroviral therapy in India: starting criteria and second-line therapy
Abstract
Background: India has more than 5.7 million people infected with human immunodeficiency virus (HIV). In 2004, the Indian government began providing antiretroviral therapy (ART), and there are now an estimated 56 500 people receiving ART.
Objective: To project the life expectancy, cost, and cost-effectiveness associated with different strategies for using ART in India, to inform treatment programs.
Methods: We utilized an HIV disease simulation model, incorporating data on natural history, treatment efficacy, and costs of care from India. Input parameters for the simulated cohort included mean age 32.6 years and mean CD4 count 318 cells/microl (SD 291 cells/microl). We examined different criteria for starting and stopping ART with a first-line regimen of stavudine/lamivudine/nevirapine, and the impact of a second-line protease-inhibitor-based regimen. Cost-effectiveness in US dollars per year of life saved (US$/YLS) was compared incrementally among alternative starting, sequencing, and stopping criteria.
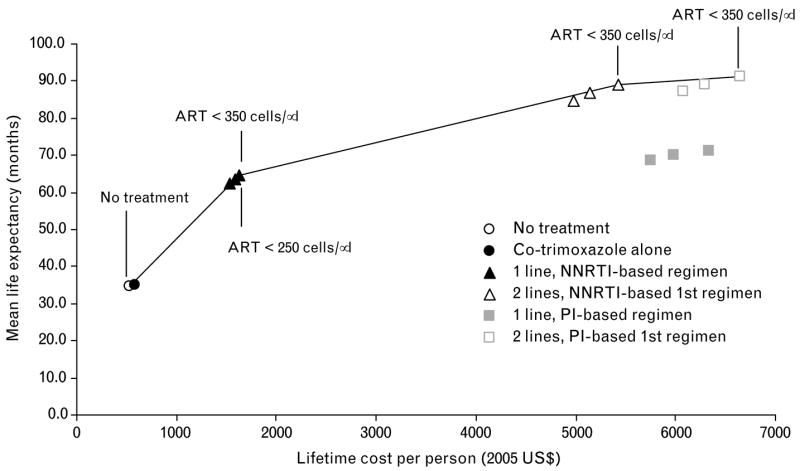
Results: Discounted (undiscounted) mean survival ranged from 34.5 (37.5) months with no ART to 64.7 (73.6) months with one line of therapy initiated at CD4 <350 cells/microl, to 88.9 (106.5) months with two lines of therapy initiated at CD4 <350 cells/microl. Lifetime medical costs ranged from US$530 (no ART) to US$5430 (two ART regimens) per person. With one line of therapy, the incremental cost-effectiveness ratios ranged from US$430/YLS to US$550/YLS as the CD4 starting criterion was increased from CD4 <250 cells/microl to <350 cells/microl. Use of two lines of therapy had an incremental cost-effectiveness ratio of US$1880/YLS compared with the use of first-line therapy alone. Results were sensitive to the costs of second-line therapy and criteria for stopping therapy.
Conclusions: In India, antiretroviral therapy will lead to major survival benefits and is cost-effective by World Health Organization criteria. The availability of second-line regimens will further increase survival, but their cost-effectiveness depends on their relative cost compared with first-line regimens.
Figures
References
-
- WHO. Summary country profile for HIV/AIDS treatment scale-up: India. [Accessed: 30 March 2007]. http://www.who.int/hiv/HIVCP_IND.pdf.
-
- UNAIDS/WHO. AIDS epidemic update: special report on HIV/AIDS: December 2006. [Accessed: 30 March 2007]. http://www.unaids.org/en/HIV_data/epi2006/default.asp.
-
- Kumarasamy N, Solomon S, Chaguturu SK, Cecelia AJ, Vallabhaneni S, Flanigan TP, Mayer KH. The changing natural history of HIV disease: before and after the introduction of generic antiretroviral therapy in southern India. Clin Infect Dis. 2005;41:1525–1528. - PubMed
-
- Steinbrook R. HIV in India – the challenges ahead. N Engl J Med. 2007;356:1197–1201. - PubMed
-
- National AIDS Control Organization, Ministry of Health and Family Welfare, India Go. National guidelines for implementation of antiretroviral therapy (ART) [Accessed: 30 March 2007]. http://www.nacoonline.org/guidelines/ART_Guidelines.pdf.
Publication types
MeSH terms
Substances
Grants and funding
- U01 AI 38858/AI/NIAID NIH HHS/United States
- K23 AI001794/AI/NIAID NIH HHS/United States
- K23 AI 01794/AI/NIAID NIH HHS/United States
- U01 AI038858/AI/NIAID NIH HHS/United States
- T32 AI 07433/AI/NIAID NIH HHS/United States
- R01 AI 058736/AI/NIAID NIH HHS/United States
- K25 AI 50436/AI/NIAID NIH HHS/United States
- R01 AI058736/AI/NIAID NIH HHS/United States
- T32 AI007433/AI/NIAID NIH HHS/United States
- P30 AI060354/AI/NIAID NIH HHS/United States
- K25 AI050436/AI/NIAID NIH HHS/United States
- P30 AI 60354/AI/NIAID NIH HHS/United States
- K24 AI 062476/AI/NIAID NIH HHS/United States
- K24 AI062476/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
