

Neuroendocrine-immune disequilibrium and endometriosis: an interdisciplinary approach
- PMID: 17621704
- PMCID: PMC2668599
- DOI: 10.1007/s00281-007-0077-0
Neuroendocrine-immune disequilibrium and endometriosis: an interdisciplinary approach
Abstract
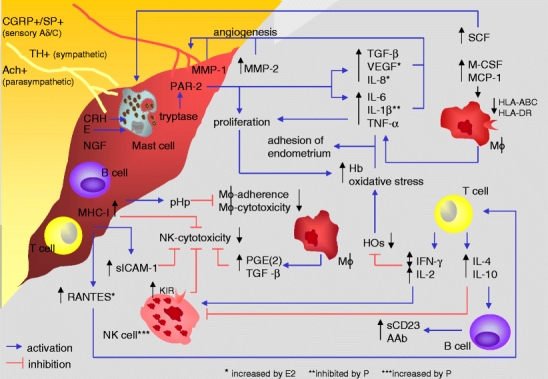
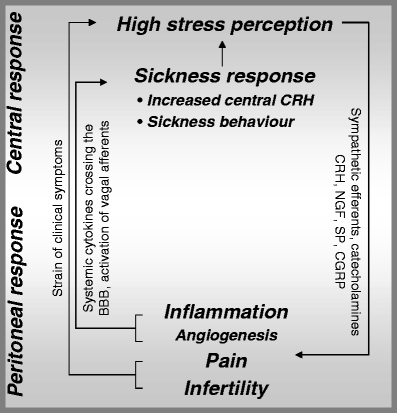
Endometriosis, a chronic disease characterized by endometrial tissue located outside the uterine cavity, affects one fourth of young women and is associated with chronic pelvic pain and infertility. However, an in-depth understanding of the pathophysiology and effective treatment strategies of endometriosis is still largely elusive. Inadequate immune and neuroendocrine responses are significantly involved in the pathophysiology of endometriosis, and key findings are summarized in the present review. We discuss here the role of different immune mechanisms particularly adhesion molecules, proteinglycan interactions, and pro-angiogenic mediators in the development and progression of the disease. Finally, we introduce the concept of endometrial dissemination as result of a neuroendocrine-immune disequilibrium in response to high levels of perceived stress caused by cardinal clinical symptoms of endometriosis.
Figures
References
-
- None
- Rokitansky K (1860) Über Uterusdrüsen-Neubildung. Z Gesellschaft Aerzte (Wien) 16:577–581
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '1939552', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/1939552/'}]}
- Moen MH, Muus KM (1991) Endometriosis in pregnant and non-pregnant women at tubal sterilization. Hum Reprod 6:699–702 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '2010001', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/2010001/'}]}
- Koninckx PR, Meuleman C, Demeyere S, Lesaffre E, Cornillie FJ (1991) Suggestive evidence that pelvic endometriosis is a progressive disease, whereas deeply infiltrating endometriosis is associated with pelvic pain. Fertil Steril 55:759–765 - PubMed
-
- None
- Bruckner C (2004) Symptoms and diagnosis. In: Steck T, Felberbaum R, Küpker W, Bruckner C, Finas D (eds) Endometriosis. Development, diagnosis, progression, therapy. Springer, New York, pp 81–101
-
- None
- Steck T (2004) Manifestations and progression. In: Steck T, Felberbaum R, Küpker W, Bruckner C, Finas D (eds) Endometriosis. Development, diagnosis, progression, therapy. Springer, Berlin Heidelberg New York, pp 37–79
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
