

Endovascular repair of paraanastomotic aneurysms after aortic reconstruction
- PMID: 17622359
- PMCID: PMC1894696
Endovascular repair of paraanastomotic aneurysms after aortic reconstruction
Abstract
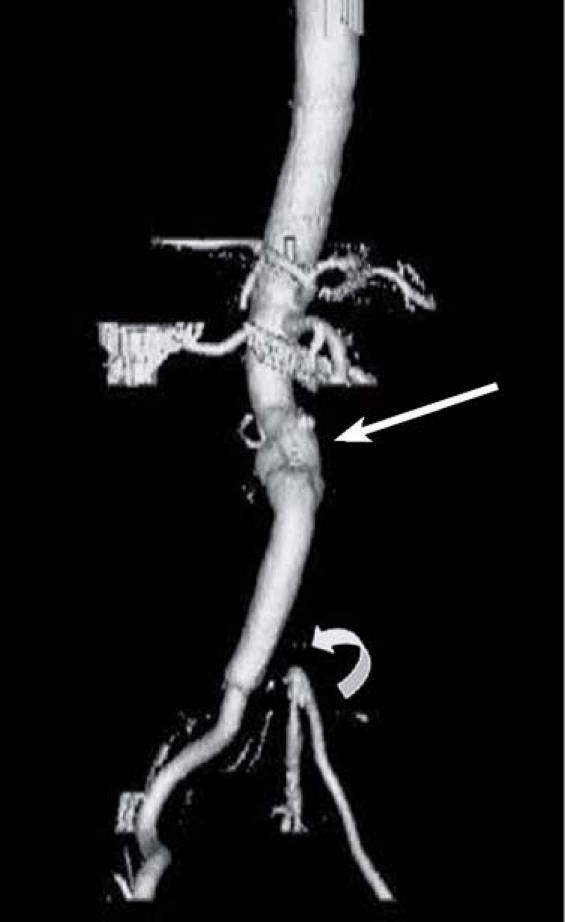
We designed this retrospective study to evaluate the effectiveness of percutaneous approaches for repair of paraanastomotic aneurysms that develop after surgical aortic reconstruction. The catheterization records of patients who had undergone percutaneous repair of para-anastomotic aneurysms from January 2001 through December 2005 were reviewed, and data regarding preoperative aneurysm size, risk factors, intraoperative techniques, morbidity, and death were recorded. Eight patients had undergone exclusion of a total of 10 paraanastomotic aneurysms. The average age of the prosthetic graft at diagnosis was 11.7 years. Four of the patients were symptomatic; none of these had a ruptured aneurysm. All patients received commercially available devices. Technical success was achieved in all patients. Conscious sedation alone was administered to 7 patients. There were no in-hospital deaths, and morbidity was minimal. We conclude that endovascular exclusion of paraanastomotic aneurysms after aortic reconstruction is a viable alternative to open surgical repair and greatly reduces the risk of morbidity and death.
Figures



Similar articles
-
Endovascular repair of paraanastomotic aneurysms after previous open aortic prosthetic reconstruction.Ann Vasc Surg. 2004 May;18(3):280-6. doi: 10.1007/s10016-004-0002-0. Ann Vasc Surg. 2004. PMID: 15354628
-
Endovascular repair of a paraanastomotic aneurysm with inverted limb infrarenal bifurcated graft.Ann Vasc Surg. 2014 Feb;28(2):493.e5-10. doi: 10.1016/j.avsg.2013.03.019. Epub 2013 Dec 2. Ann Vasc Surg. 2014. PMID: 24295882
-
Endovascular repair of postoperative vascular graft related complications after aorto-iliac surgery.Int Angiol. 2014 Aug;33(4):386-91. Int Angiol. 2014. PMID: 25056171
-
Intentional Bilateral Renal Artery Coverage During Ruptured Endovascular Paraanastomotic Pseudoaneurysm Repair.Ann Vasc Surg. 2022 Feb;79:440.e1-440.e6. doi: 10.1016/j.avsg.2021.07.040. Epub 2021 Oct 12. Ann Vasc Surg. 2022. PMID: 34653639 Review.
-
Aortic anastomosis surveillance.Eur J Vasc Endovasc Surg. 1997 Dec;14 Suppl A:30-4. doi: 10.1016/s1078-5884(97)80150-5. Eur J Vasc Endovasc Surg. 1997. PMID: 9467611 Review. No abstract available.
Cited by
-
Precision Medicine in Aortic Anastomosis: A Numerical and Experimental Study of a Novel Double-Sided Needle.J Pers Med. 2021 Dec 20;11(12):1385. doi: 10.3390/jpm11121385. J Pers Med. 2021. PMID: 34945857 Free PMC article.
-
Embolization with Histoacryl Glue of an Anastomotic Pseudoaneurysm following Surgical Repair of Abdominal Aortic Aneurysm.Case Rep Vasc Med. 2013;2013:761384. doi: 10.1155/2013/761384. Epub 2013 Feb 12. Case Rep Vasc Med. 2013. PMID: 23476883 Free PMC article.
-
Endovascular stent-grafting of anastomotic pseudoaneurysms following thoracic aortic surgery.Gen Thorac Cardiovasc Surg. 2009 Oct;57(10):528-33. doi: 10.1007/s11748-009-0477-2. Epub 2009 Oct 16. Gen Thorac Cardiovasc Surg. 2009. PMID: 19830515
-
"To-and-fro" waveform in the diagnosis of arterial pseudoaneurysms.World J Radiol. 2015 May 28;7(5):89-99. doi: 10.4329/wjr.v7.i5.89. World J Radiol. 2015. PMID: 26029351 Free PMC article. Review.
-
[Endovascular therapy of para-anastomotic aneurysms of the aorta. Technical options].Chirurg. 2013 Oct;84(10):881-8. doi: 10.1007/s00104-013-2486-z. Chirurg. 2013. PMID: 23564196 Review. German.
References
-
- Curl GR, Faggioli GL, Ricotta JJ. Proximal para-anastomotic aortic aneurysm. In: Veith FJ, editor. Current critical problems in vascular surgery. Vol 5. St. Louis: Quality Medical Publishing; 1993. p. 240–6.
-
- Allen RC, Schneider J, Longenecker L, Smith RB 3rd, Lumsden AB. Paraanastomotic aneurysms of the abdominal aorta. J Vasc Surg 1993;18:424–32. - PubMed
-
- Sonesson B, Resch T, Lanne T, Ivancev K. The fate of the infrarenal aortic neck after open aneurysm surgery. J Vasc Surg 1998;28:889–94. - PubMed
-
- Starr DS, Weatherford SC, Lawrie GM, Morris GC Jr. Suture material as a factor in the occurrence of anastomotic false aneurysms. An analysis of 26 cases. Arch Surg 1979;114:412–5. - PubMed
-
- Curl GR, Faggioli GL, Stella A, D'Addato M, Ricotta JJ. Aneurysmal change at or above the proximal anastomosis after infrarenal aortic grafting. J Vasc Surg 1992;16:855–60. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources