

Friedreich's ataxia as a cause of premature coronary artery disease
- PMID: 17622372
- PMCID: PMC1894724
Friedreich's ataxia as a cause of premature coronary artery disease
Abstract
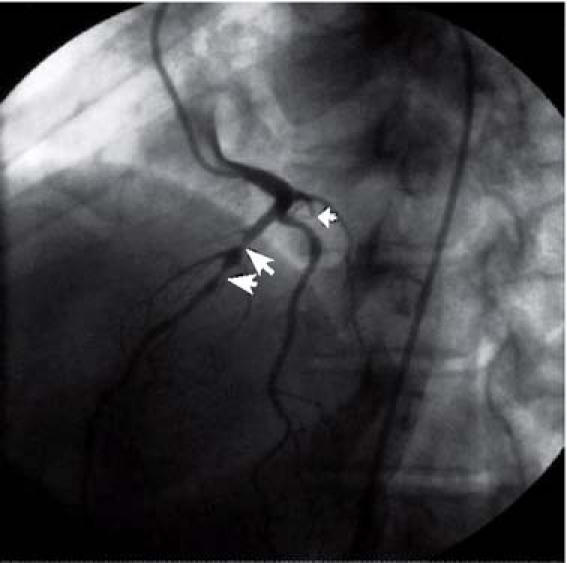
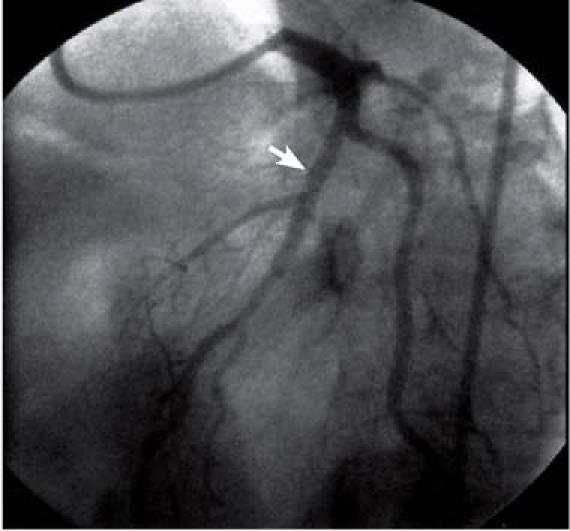
Friedreich's ataxia is the most common hereditary neurodegenerative disorder, and more than half of all patients show echocardiographic evidence of cardiomyopathy. Although angina has been reported in these patients, the role of coronary artery disease has previously been dismissed and is therefore underestimated. Premature obstructive coronary disease has rarely been angiographically demonstrated in patients with Friedreich's ataxia. We present an unusual case of a 35-year-old woman with Friedreich's ataxia who presented with intermittent chest pressure associated with dyspnea and diaphoresis. Cardiac catheterization revealed a chronically occluded left circumflex coronary artery and a high-grade stenosis of the left anterior descending coronary artery. A Cypher stent, placed within the left anterior descending artery, left no residual stenosis. This case illustrates the importance of fully investigating anginal symptoms in patients with Friedreich's ataxia, because coronary artery disease is likely underdiagnosed in this population. Early diagnosis may permit aggressive management and may delay the progression to end-stage cardiomyopathy.
Figures

Comment in
-
Mortality in Friedreich's Ataxia.Tex Heart Inst J. 2007;34(4):502-3; author reply 503-4. Tex Heart Inst J. 2007. PMID: 18172544 Free PMC article. No abstract available.
References
-
- Alboliras ET, Shub C, Gomez MR, Edwards WD, Hagler DJ, Reeder GS, et al. Spectrum of cardiac involvement in Friedreich's ataxia: clinical, electrocardiographic and echocardiographic observations. Am J Cardiol 1986;58:518–24. - PubMed
-
- Campuzano V, Montermini L, Molto MD, Pianese L, Cossee M, Cavalcanti F, et al. Friedreich's ataxia: autosomal recessive disease caused by an intronic GAA triplet repeat expansion. Science 1996;271:1423–7. - PubMed
-
- Schols L, Meyer CH, Schmid G, Wilhelms I, Przuntek H. Therapeutic strategies in Friedreich's ataxia. J Neural Transm Suppl 2004;68:135–45. - PubMed
-
- Groh WJ, Zipes DP. Neurological disorders and cardiovascular disease. In: Zipes DP, Libby P, Bonow RO, Braunwald E, editors. Braunwald's heart disease: a textbook of cardiovascular medicine. 7th ed. Philadelphia: Elsevier Saunders; 2005. p. 2153–4.
-
- Labuda M, Labuda D, Miranda C, Poirier J, Soong BW, Barucha NE, Pandolfo M. Unique origin and specific ethnic distribution of the Friedreich ataxia GAA expansion. Neurology 2000;54:2322–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical