

Adult obstructive sleep apnea: pathophysiology and diagnosis
- PMID: 17625094
- PMCID: PMC2813513
- DOI: 10.1378/chest.07-0040
Adult obstructive sleep apnea: pathophysiology and diagnosis
Abstract
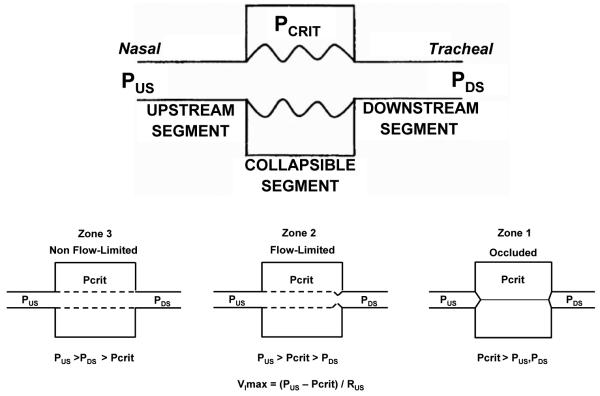
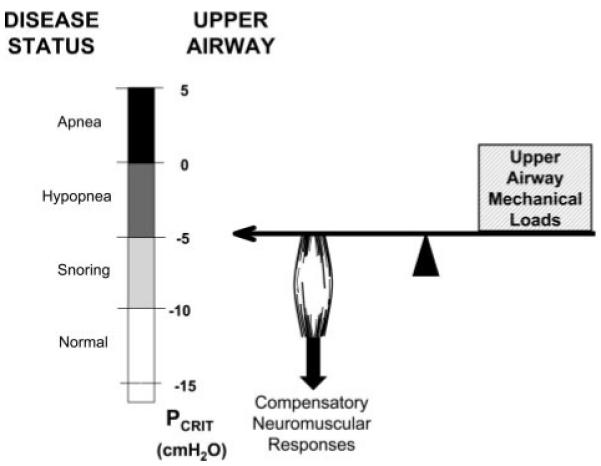
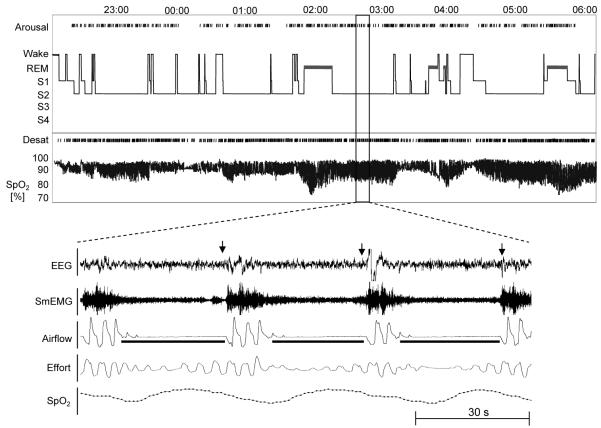
Obstructive sleep apnea (OSA) is a highly prevalent disease characterized by recurrent episodes of upper airway obstruction that result in recurrent arousals and episodic oxyhemoglobin desaturations during sleep. Significant clinical consequences of the disorder cover a wide spectrum, including daytime hypersomnolence, neurocognitive dysfunction, cardiovascular disease, metabolic dysfunction, and cor pulmonale. The major risk factors for the disorder include obesity, male gender, and age. Current understanding of the pathophysiologic basis of the disorder suggests that a balance of anatomically imposed mechanical loads and compensatory neuromuscular responses are important in maintaining upper airway patency during sleep. OSA develops in the presence of both elevated mechanical loads on the upper airway and defects in compensatory neuromuscular responses. A sleep history and physical examination is important in identification of patients and appropriate referral for polysomnography. Understanding nuances in the spectrum of presenting complaints and polysomnography correlates are important for diagnostic and therapeutic approaches. Knowledge of common patterns of OSA may help to identify patients and guide therapy.
Figures


References
-
- Young T, Palta M, Dempsey J, et al. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328:1230–1235. - PubMed
-
- Remmers JE, deGroot WJ, Sauerland EK, et al. Pathogenesis of upper airway occlusion during sleep. J Appl Physiol. 1978;44:931–938. - PubMed
-
- Punjabi NM, Bandeen-Roche K, Marx JJ, et al. The association between daytime sleepiness and sleep-disordered breathing in NREM and REM sleep. Sleep. 2002;25:307–314. - PubMed
-
- Punjabi NM, O’Hearn DJ, Neubauer DN, et al. Modeling hypersomnolence in sleep-disordered breathing: a novel approach using survival analysis. Am J Respir Crit Care Med. 1999;159:1703–1709. - PubMed
-
- Adams N, Strauss M, Schluchter M, et al. Relation of measures of sleep-disordered breathing to neuropsychological functioning. Am J Respir Crit Care Med. 2001;163:1626–1631. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
