

Transfusion-related acute lung injury in the critically ill: prospective nested case-control study
- PMID: 17626910
- PMCID: PMC2048675
- DOI: 10.1164/rccm.200702-271OC
Transfusion-related acute lung injury in the critically ill: prospective nested case-control study
Abstract
Rationale: Acute lung injury (ALI) that develops 6 hours after transfusion (TRALI) is the leading cause of transfusion-related mortality. Several transfusion characteristics have been postulated as risk factors for TRALI, but the evidence is limited to retrospective studies.
Objectives: To compare patient and transfusion risk factors between patients who do and do not develop ALI.
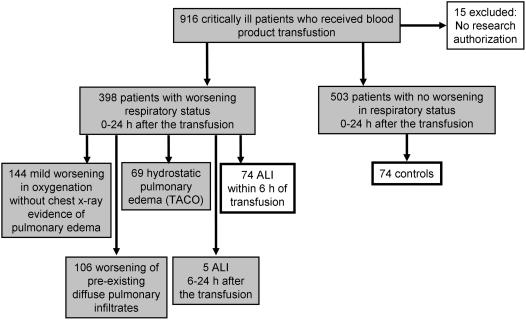
Methods: In this prospective cohort study, consecutive transfused critically ill patients were closely observed for development of ALI. Donor samples were collected from the transfusion bags. Risk factors were compared between patients who developed ALI after transfusion and transfused control patients, matched by age, sex, and admission diagnosis.
Measurements and main results: Seventy-four of 901 transfused patients developed ALI within 6 hours of transfusion (8%). Compared with transfused control subjects, patients with ALI were more likely to have sepsis (37 vs. 22%, P = 0.016) and a history of chronic alcohol abuse (37 vs. 18%, P = 0.006). When adjusted for patient characteristics, transfusion of plasma from female donors (odds ratio [OR], 5.09; 95% confidence interval [95% CI], 1.37-18.85) rather than male donors (OR, 1.60; 95% CI, 0.76 to 3.37), number of pregnancies among the donors (OR, 1.19; 95% CI, 1.05 to 1.34), number of donor units positive for anti-granulocyte antibodies (OR, 4.85; 95% CI, 1.32-17.86) and anti-HLA class II antibodies (OR, 3.08; 95% CI, 1.15-8.25), and concentration of lysophosphatidylcholine in the donor product (OR, 1.69; 95% CI, 1.10 to 2.59) were associated with the development of ALI.
Conclusions: Both patient and transfusion risk factors determine the probability of ALI after transfusion. Transfusion factors represent attractive targets for the prevention of ALI.
Figures
Comment in
-
TRALI: a new case definition, a new epidemic?Am J Respir Crit Care Med. 2007 Nov 1;176(9):839-40. doi: 10.1164/rccm.200708-1169ED. Am J Respir Crit Care Med. 2007. PMID: 17951557 No abstract available.
References
-
- Popovsky MA, Abel MD, Moore SB. Transfusion-related acute lung injury associated with passive transfer of antileukocyte antibodies. Am Rev Respir Dis 1983;128:185–189. - PubMed
-
- Holness L, Knippen MA, Simmons L, Lachenbruch PA. Fatalities caused by TRALI. Transfus Med Rev 2004;18:184–188. - PubMed
-
- Toy P, Popovsky MA, Abraham E, Ambruso DR, Holness LG, Kopko PM, McFarland JG, Nathens AB, Silliman CC, Stroncek D. Transfusion-related acute lung injury: definition and review. Crit Care Med 2005;33:721–726. - PubMed
-
- Kleinman S, Caulfield T, Chan P, Davenport R, McFarland J, McPhedran S, Meade M, Morrison D, Pinsent T, Robillard P, et al. Toward an understanding of transfusion-related acute lung injury: statement of a consensus panel. Transfusion 2004;44:1774–1789. - PubMed
-
- Kopko PM, Marshall CS, MacKenzie MR, Holland PV, Popovsky MA. Transfusion-related acute lung injury: report of a clinical look-back investigation. JAMA 2002;287:1968–1971. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
