

Prognostic implications of relations of left ventricular systolic dysfunction with body composition and myocardial energy expenditure: the Strong Heart Study
- PMID: 17628407
- PMCID: PMC4294423
- DOI: 10.1016/j.echo.2007.05.008
Prognostic implications of relations of left ventricular systolic dysfunction with body composition and myocardial energy expenditure: the Strong Heart Study
Abstract
Objective: We sought to investigate prognostic implications of the relationships of estimated left ventricular (LV) myocardial energy expenditure (MEE) with LV systolic dysfunction, body composition, and inflammation in a population-based sample of adults without overt congestive heart failure.
Methods: Echocardiography was used to assess LV ejection fraction (EF) and MEE. Body composition was evaluated by bioelectric impedance. Dietary recall was used to assess 24-hour calorie intake. Participants in the Strong Heart Study without prior congestive heart failure and with all needed data available (n = 3087) were divided based on LV EF (>55%, 54%-45%, or <45%).
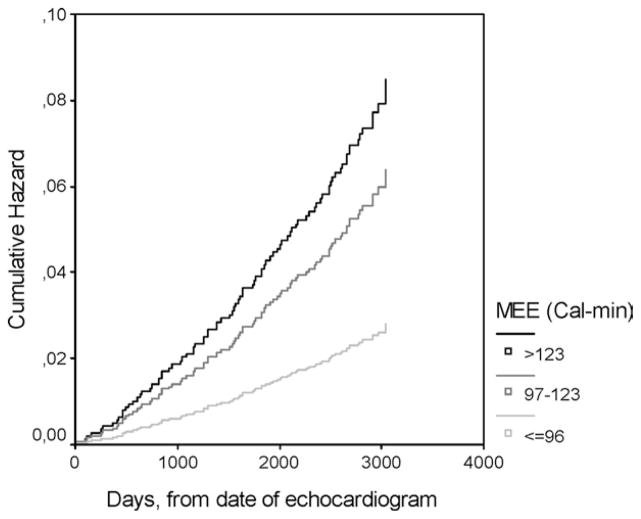
Results: Participants with EF less than 45% were older and they had lower body mass index, adipose mass, fat-free mass, and 24-hour calorie intake than participants with normal EF (>/=55%), and had greatest reductions of body mass index and physical activity in a time interval of 3.5 years, on average, elapsed between an initial clinical assessment and the evaluation at the time of the echocardiographic examination (P < .01). Lower EF was associated with male sex, hypertension, diabetes, coronary heart disease, and higher fibrinogen, C-reactive protein, and plasma creatinine levels (all P < .01). MEE was higher with lower EF (all P < .001). In Cox regression models, during approximately 8 years of observation, MEE comprised between 97 and 123 cal/min and MEE greater than 123 cal/min were associated with 2.5-fold and additional 3.3-fold higher rates of cardiac death, respectively, compared with MEE less than 97 cal/min, independently of EF, body composition, and other covariates. However, lower adipose mass predicted increased risk of cardiac death independent of MEE and EF.
Conclusion: In a population-based sample of adults including ambulatory individuals with depressed LV systolic function but without overt congestive heart failure, depressed EF was associated independently with higher MEE, lower adipose mass, and higher fibrinogen. However, increased MEE and lower adipose mass predicted cardiac death independently of EF and other covariates.
Figures
Similar articles
-
Prognostic implications of ejection fraction from linear echocardiographic dimensions: the Strong Heart Study.Am Heart J. 2003 Sep;146(3):527-34. doi: 10.1016/S0002-8703(03)00229-1. Am Heart J. 2003. PMID: 12947374
-
Utility of the myocardial performance index in a population with high prevalences of obesity, diabetes, and hypertension: the strong heart study.Echocardiography. 2007 Apr;24(4):340-7. doi: 10.1111/j.1540-8175.2007.00415.x. Echocardiography. 2007. PMID: 17381641
-
Influence of Left Ventricular Stroke Volume on Incident Heart Failure in a Population With Preserved Ejection Fraction (from the Strong Heart Study).Am J Cardiol. 2017 Apr 1;119(7):1047-1052. doi: 10.1016/j.amjcard.2016.12.011. Epub 2017 Jan 5. Am J Cardiol. 2017. PMID: 28159195 Free PMC article.
-
Clinical aspects of left ventricular diastolic function assessed by Doppler echocardiography following acute myocardial infarction.Dan Med Bull. 2001 Nov;48(4):199-210. Dan Med Bull. 2001. PMID: 11767125 Review.
-
Depressed Cardiac Mechanical Energetic Efficiency: A Contributor to Cardiovascular Risk in Common Metabolic Diseases-From Mechanisms to Clinical Applications.J Clin Med. 2020 Aug 19;9(9):2681. doi: 10.3390/jcm9092681. J Clin Med. 2020. PMID: 32824903 Free PMC article. Review.
Cited by
-
Right Ventricular Dysfunction Impairs Effort Tolerance Independent of Left Ventricular Function Among Patients Undergoing Exercise Stress Myocardial Perfusion Imaging.Circ Cardiovasc Imaging. 2016 Nov;9(11):e005115. doi: 10.1161/CIRCIMAGING.116.005115. Circ Cardiovasc Imaging. 2016. PMID: 27903538 Free PMC article.
-
The Value of Myocardial Energy Expenditure in the Diagnosis of Cirrhotic Cardiomyopathy.Int J Gen Med. 2025 Jul 5;18:3767-3774. doi: 10.2147/IJGM.S529946. eCollection 2025. Int J Gen Med. 2025. PMID: 40636287 Free PMC article.
-
Relationship between myocardial energy expenditure and postoperative ejection fraction in patients with severe mitral regurgitation.Anatol J Cardiol. 2020 Oct;24(4):254-259. doi: 10.14744/AnatolJCardiol.2020.03835. Anatol J Cardiol. 2020. PMID: 33001042 Free PMC article.
-
Effect of granulocyte colony stimulating EPC on cardiac function and myocardial energy expenditure in patients with heart failure after myocardial infarction.Int J Clin Exp Med. 2015 Sep 15;8(9):16578-84. eCollection 2015. Int J Clin Exp Med. 2015. PMID: 26629187 Free PMC article.
-
Recent advances in the diagnosis and management of cirrhosis-associated cardiomyopathy in liver transplant candidates: advanced echo imaging, cardiac biomarkers, and advanced heart failure therapies.Clin Med Insights Cardiol. 2015 Jan 28;8(Suppl 1):67-74. doi: 10.4137/CMC.S15722. eCollection 2014. Clin Med Insights Cardiol. 2015. PMID: 25657603 Free PMC article. Review.
References
-
- Calle EE, Thun MJ, Petrelli JM, Rodriguez C, Heath CW., Jr Body-mass index and mortality in a prospective cohort of US adults. N Engl J Med. 1999;341:1097–105. - PubMed
-
- de Simone G, Wachtell K, Palmieri V, Hille DA, Beevers G, Dahlof B, et al. Body build and risk of cardiovascular events in hypertension and left ventricular hypertrophy: the LIFE (losartan intervention for endpoint reduction in hypertension) study. Circulation. 2005;111:1924–31. - PubMed
-
- Lavie CJ, Osman AF, Milani RV, Mehra MR. Body composition and prognosis in chronic systolic heart failure: the obesity paradox. Am J Cardiol. 2003;91:891–4. - PubMed
-
- Davos CH, Doehner W, Rauchhaus M, Cicoira M, Francis DP, Coats AJ, et al. Body mass and survival in patients with chronic heart failure without cachexia: the importance of obesity. J Card Fail. 2003;9:29–35. - PubMed
-
- Curtis JP, Selter JG, Wang Y, Rathore SS, Jovin IS, Jadbabaie F, et al. The obesity paradox: body mass index and outcomes in patients with heart failure. Arch Intern Med. 2005;165:55–61. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
