

Quality of life before intensive care unit admission is a predictor of survival
- PMID: 17629906
- PMCID: PMC2206516
- DOI: 10.1186/cc5970
Quality of life before intensive care unit admission is a predictor of survival
Abstract
Introduction: Predicting whether a critically ill patient will survive intensive care treatment remains difficult. The advantages of a validated strategy to identify those patients who will not benefit from intensive care unit (ICU) treatment are evident. Providing critical care treatment to patients who will ultimately die in the ICU is accompanied by an enormous emotional and physical burden for both patients and their relatives. The purpose of the present study was to examine whether health-related quality of life (HRQOL) before admission to the ICU can be used as a predictor of mortality.
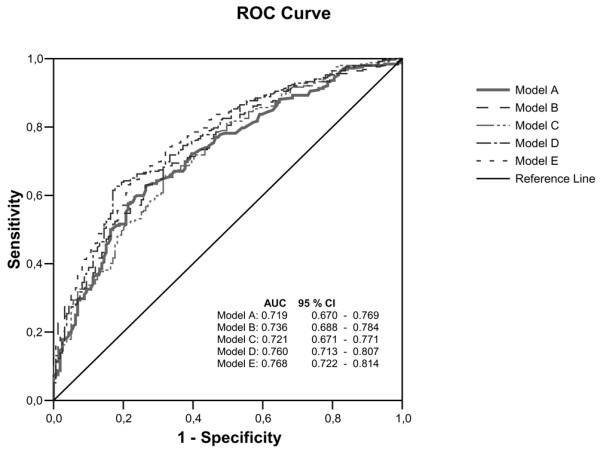
Methods: We conducted a prospective cohort study in a university-affiliated teaching hospital. Patients admitted to the ICU for longer than 48 hours were included. Close relatives completed the Short-form 36 (SF-36) within the first 48 hours of admission to assess pre-admission HRQOL of the patient. Mortality was evaluated from ICU admittance until 6 months after ICU discharge. Logistic regression and receiver operating characteristic analyses were used to assess the predictive value for mortality using five models: the first question of the SF-36 on general health (model A); HRQOL measured using the physical component score (PCS) and mental component score (MCS) of the SF-36 (model B); the Acute Physiology and Chronic Health Evaluation (APACHE) II score (an accepted mortality prediction model in ICU patients; model C); general health and APACHE II score (model D); and PCS, MCS and APACHE II score (model E). Classification tables were used to assess the sensitivity, specificity, positive and negative predictive values, and likelihood ratios.
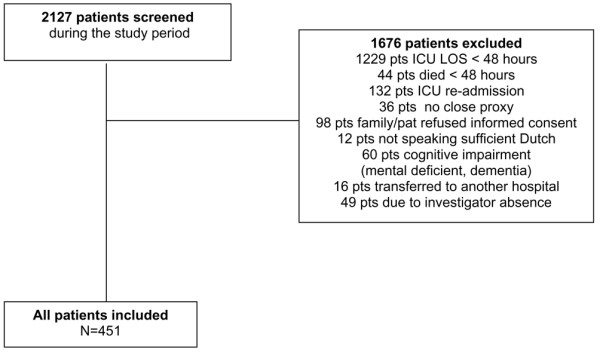
Results: A total of 451 patients were included within 48 hours of admission to the ICU. At 6 months of follow up, 159 patients had died and 40 patients were lost to follow up. When the general health item was used as an estimate of HRQOL, area under the curve for model A (0.719) was comparable to that of model C (0.721) and slightly better than that of model D (0.760). When PCS and MCS were used, the area under the curve for model B (0.736) was comparable to that of model C (0.721) and slightly better than that of model E (0.768). When using the general health item, the sensitivity and specificity in model D (sensitivity 0.52 and specificity 0.81) were similar to those in model A (0.45 and 0.80). Similar results were found when using the MCS and PCS.
Conclusion: This study shows that the pre-admission HRQOL measured with either the one-item general health question or the complete SF-36 is as good at predicting survival/mortality in ICU patients as the APACHE II score. The value of these measures in clinical practice is limited, although it seems sensible to incorporate assessment of HRQOL into the many variables considered when deciding whether a patient should be admitted to the ICU.
Figures
Similar articles
-
The acute physiology and chronic health evaluation III outcome prediction in patients admitted to the intensive care unit after pneumonectomy.J Cardiothorac Vasc Anesth. 2007 Dec;21(6):832-7. doi: 10.1053/j.jvca.2006.12.005. Epub 2007 Mar 6. J Cardiothorac Vasc Anesth. 2007. PMID: 18068061
-
The outcome of acute renal failure in the intensive care unit according to RIFLE: model application, sensitivity, and predictability.Am J Kidney Dis. 2005 Dec;46(6):1038-48. doi: 10.1053/j.ajkd.2005.08.033. Am J Kidney Dis. 2005. PMID: 16310569 Clinical Trial.
-
Acute Physiology and Chronic Health Evaluation (APACHE) IV: hospital mortality assessment for today's critically ill patients.Crit Care Med. 2006 May;34(5):1297-310. doi: 10.1097/01.CCM.0000215112.84523.F0. Crit Care Med. 2006. PMID: 16540951
-
Performance of prognostic models in critically ill cancer patients - a review.Crit Care. 2005 Aug;9(4):R458-63. doi: 10.1186/cc3765. Epub 2005 Jul 8. Crit Care. 2005. PMID: 16137361 Free PMC article. Review.
-
Predicting outcomes for cardiac surgery patients after intensive care unit admission.Semin Cardiothorac Vasc Anesth. 2008 Sep;12(3):175-83. doi: 10.1177/1089253208323413. Semin Cardiothorac Vasc Anesth. 2008. PMID: 18805852 Review.
Cited by
-
Quality of life before surgical ICU admission.BMC Surg. 2007 Nov 12;7:23. doi: 10.1186/1471-2482-7-23. BMC Surg. 2007. PMID: 17997828 Free PMC article.
-
Factors influencing pre-stroke and post-stroke quality of life among stroke survivors in a lower middle-income country.Neurol Sci. 2018 Feb;39(2):287-295. doi: 10.1007/s10072-017-3172-6. Epub 2017 Nov 4. Neurol Sci. 2018. PMID: 29103178
-
Does intensive care unit severity of illness influence recall of baseline physical function?J Crit Care. 2011 Dec;26(6):634.e1-7. doi: 10.1016/j.jcrc.2011.05.009. Epub 2011 Jul 6. J Crit Care. 2011. PMID: 21737233 Free PMC article.
-
Long-term mortality and quality of life after septic shock: a follow-up observational study.Intensive Care Med. 2013 May;39(5):881-8. doi: 10.1007/s00134-013-2815-1. Epub 2013 Jan 29. Intensive Care Med. 2013. PMID: 23358541
-
Quality of life and persisting symptoms in intensive care unit survivors: implications for care after discharge.BMC Res Notes. 2009 Aug 12;2:160. doi: 10.1186/1756-0500-2-160. BMC Res Notes. 2009. PMID: 19674457 Free PMC article.
References
-
- Knaus WA, Wagner DP, Zimmerman JE, Draper EA. Variations in mortality and length of stay in intensive care units. Ann Intern Med. 1993;118:753–761. - PubMed
-
- Reis Miranda D, Gyldmark M. Evaluating and Understanding of Costs in the Intensive Care Unit. In: Ryan DW, editor. Current practice in Critical Illness. London: Chapman & Hall; 1996. pp. 129–149.
MeSH terms
LinkOut - more resources
Full Text Sources
