

Pathology features in Bethesda guidelines predict colorectal cancer microsatellite instability: a population-based study
- PMID: 17631130
- PMCID: PMC2933045
- DOI: 10.1053/j.gastro.2007.04.044
Pathology features in Bethesda guidelines predict colorectal cancer microsatellite instability: a population-based study
Abstract
Background & aims: The revised Bethesda guidelines for Lynch syndrome recommend microsatellite instability (MSI) testing all colorectal cancers in patients diagnosed before age 50 years and colorectal cancers diagnosed in patients between ages 50 and 59 years with particular pathology features. Our aim was to identify pathology and other features that independently predict high MSI (MSI-H).
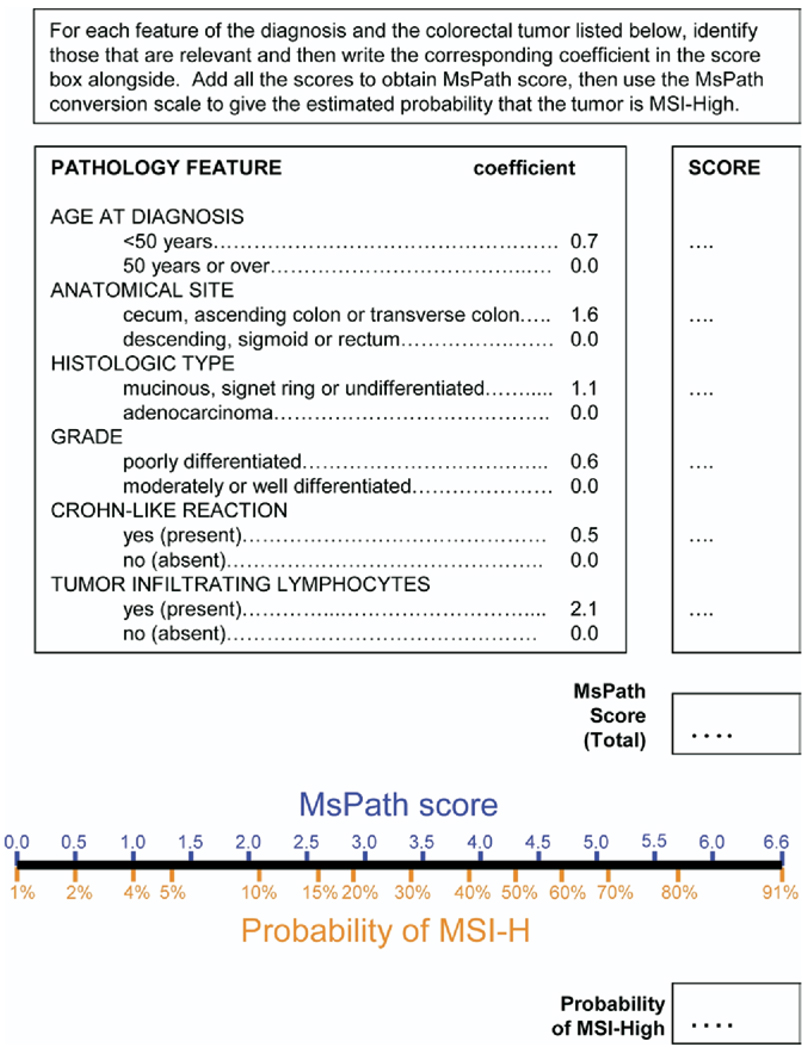
Methods: Archival tissue from 1098 population-based colorectal cancers diagnosed before age 60 years was tested for MSI. Pathology features, site, and age at diagnosis were obtained. Multiple logistic regression was performed to determine the predictive value of each feature, as measured by an odds ratio (OR), from which a scoring system (MsPath) was developed to estimate the probability a colorectal cancer is MSI-H.
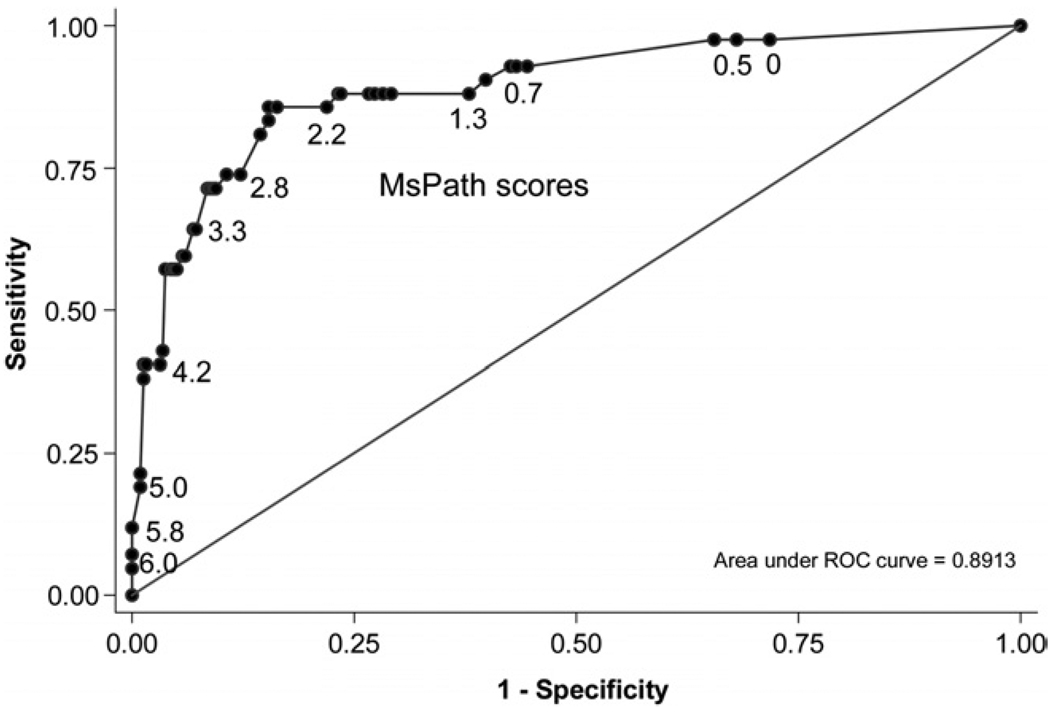
Results: Fifteen percent of tumors (162) were MSI-H. Independent predictors were tumor-infiltrating lymphocytes (OR, 9.1; 95% confidence interval [CI], 5.9-14.1), proximal subsite (OR, 4.7; 95% CI, 3.1-7.3), mucinous histology (OR, 2.8; 95% CI, 1.7-4.8), poor differentiation (OR, 1.9; 95% CI, 1.2-3.1), Crohn's-like reaction (OR, 1.9; 95% CI, 1.2-2.9), and diagnosis before age 50 years (OR, 1.9; 95% CI, 1.3-2.9). MsPath score >or=1.0 had a sensitivity of 93% and a specificity of 55% for MSI-H.
Conclusions: The probability an individual colorectal cancer is MSI-H is predicted well by the MsPath score. There is little value in testing for DNA mismatch repair loss in tumors, or for germline mismatch repair mutations, for colorectal cancers diagnosed in patients before age 60 years with an MSPath score <1 (approximately 50%). Pathology can identify almost all MSI-H colorectal cancers diagnosed before age 60 years.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Lynch HT, Smyrk T, Lynch JF. Overview of natural history, pathology, molecular genetics and mangement of HNPCC (Lynch syndrome) Int J Cancer. 1996;69:38–43. - PubMed
-
- Peltomäki P, Vasen HFA The International Collaborative Group on Hereditary Nonpolyposis Colorectal Cancer. Mutations predisposing to hereditary nonpolyposis colorectal cancer: database and results of a collaborative study. Gastroenterology. 1997;113:1146–1158. - PubMed
-
- Järvinen HJ, Aarnio M, Mustonen H, Aktan-Collan K, Aaltonen LA, Peltomaki P, De La Chapelle A, Mecklin JP. Controlled 15-year trial on screening for colorectal cancer in families with hereditary nonpolyposis colorectal cancer. Gastroenterology. 2000;118:829–834. - PubMed
-
- Southey MC, Jenkins MA, Mead LJ, Whitty J, Trivett M, Tesoriero AA, Smith LD, Jennings K, Grubb G, Royce SG, Walsh MD, Barker MA, Young JP, Jass JR, St John DJ, Macrae FA, Giles GG, Hopper JL. Use of molecular tumor characteristics to prioritize mismatch repair gene testing in early-onset colorectal cancer. J Clin Oncol. 2005;23:6524–6532. - PubMed
-
- Samowitz WS, Slattery ML, Kerber RA. Microsatellite instability in human colonic cancer is not a useful clinical indicator of familial colorectal cancer. Gastroenterology. 1995;109:1765–1771. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
