

Discontinuous vs. in-continuity neck dissection in carcinoma of the oral cavity. Experience of two oncologic hospitals
- PMID: 17633154
- PMCID: PMC2639987
Discontinuous vs. in-continuity neck dissection in carcinoma of the oral cavity. Experience of two oncologic hospitals
Abstract
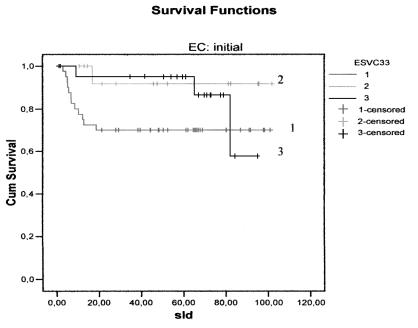
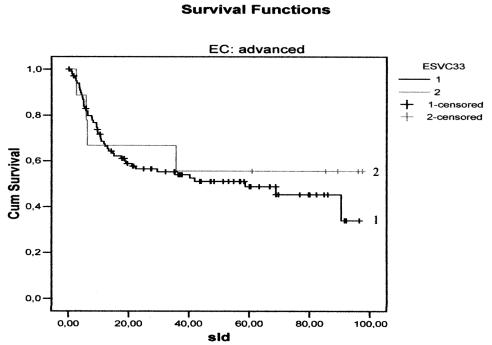
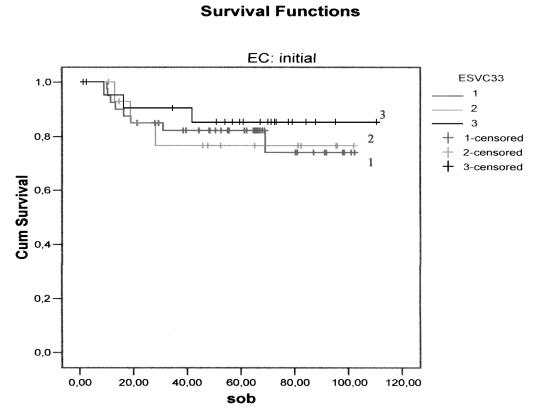
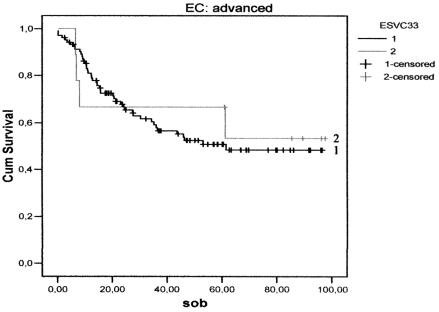
Many Authors have discussed the best indication and extension of neck dissection, but few have studied the surgical approach considering the continuity of neck dissection with the primary tumour. This retrospective study refers to patients submitted to major surgery between 1996 and 2001 for floor of mouth and oral tongue squamous cell carcinoma, at the Head and Neck Surgery Department of the Hospital "A.C. Camargo", São Paulo, Brazil and of the European Institute of Oncology, Milan, Italy. Patients were assigned to one of three groups: group I (in-continuity resection); group 2 (discontinuous resection) and group 3 (delayed discontinuous resection). Overall, 193 patients were studied. There were no differences in disease-free survival between the neck dissection groups. Furthermore, no statistical differences were found in disease specific survival between the groups. Discontinuous neck dissection seems not to change the disease-free survival or disease-specific survival when compared to in-continuity neck dissection, in this retrospective study. A prospective randomized trial is necessary to confirm these results.
Nei carcinomi della lingua e del pavimento orale l’indicazione ad una dissezione laterocervicale in blocco con la neoplasia primitiva ovvero differita è molto discussa, ed in letteratura esistono pochi contributi su questo argomento. Questo studio retrospettivo analizza i risultati di differenti atteggiamenti terapeutici sulle aree linfatiche laterocervicali in una serie di pazienti con carcinomi della lingua e del pavimento orale trattati dal 1996 al 2001 in due strutture oncologiche: l’Istituto “A. Camargo” di S. Paolo del Brasile e l’Istituto Europeo di Oncologa di Milano. I pazienti sono stati divisi in tre gruppi a seconda della tempistica dello svuotamento laterocervicale rispetto alla rimozione della neoplasia orale: 1) resezione in blocco della neoplasia con i linfonodi del collo; 2) linfoadenectomia laterocervicale sincrona ma non in continuità con la resezione della neoplasia primitiva; 3) linfoadenectomia laterocervicale differita di 30-40 giorni rispetto alla terapia della neoplasia primitiva.
Sono stati studiati globalmente 193 pazienti.
Non è stata evidenziata alcuna differenza statisticamente significativa fra i tre gruppi in termini di sopravvivenza da malattia. Sulla base di questo studio retrospettivo si può ipotizzare che le tre modalità terapeutiche di dissezione in blocco, sincrona discontinua e differita non modifichino la prognosi di pazienti con neoplasie della lingua e del pavimento orale. È necessario uno studio clinico prospettico randomizzato per confermare questa ipotesi.
Figures
Similar articles
-
Impact of elective neck dissection vs observation on regional recurrence and survival in cN0-staged patients with squamous cell carcinomas of the upper aerodigestive tract.Arch Otolaryngol Head Neck Surg. 2012 Jul;138(7):650-5. doi: 10.1001/archoto.2012.1026. Arch Otolaryngol Head Neck Surg. 2012. PMID: 22801889
-
Effectiveness of selective neck dissection in the treatment of the clinically positive neck.Head Neck. 2008 Sep;30(9):1231-6. doi: 10.1002/hed.20870. Head Neck. 2008. PMID: 18642289
-
[Selective neck dissection for node-positive necks (N1, N2) in patients with head and neck squamous cell carcinoma].Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2008 Sep;43(9):681-5. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2008. PMID: 19035262 Chinese.
-
Transoral laser resection with staged discontinuous neck dissection for oral cavity and oropharynx squamous cell carcinoma.Laryngoscope. 1995 Jan;105(1):53-60. doi: 10.1288/00005537-199501000-00013. Laryngoscope. 1995. PMID: 7837914 Review.
-
Elective supraomohyoid neck dissection for oral cavity squamous cell carcinoma: is dissection of sublevel IIB necessary?Oral Oncol. 2008 Mar;44(3):216-9. doi: 10.1016/j.oraloncology.2007.06.006. Epub 2007 Sep 7. Oral Oncol. 2008. PMID: 17826302 Review.
Cited by
-
Use of modified lateral upper arm free flap for reconstruction of soft tissue defect after resection of oral cancer.Head Face Med. 2016 Jan 29;12:9. doi: 10.1186/s13005-016-0105-1. Head Face Med. 2016. PMID: 26825783 Free PMC article.
-
Surgical management of the N0 neck in early stage T1-2 oral cancer; a personal perspective of early and late impalpable disease.Oral Maxillofac Surg. 2012 Jun;16(2):181-8. doi: 10.1007/s10006-012-0325-x. Epub 2012 May 13. Oral Maxillofac Surg. 2012. PMID: 22581159 Review.
-
Exclusive tongue tip reconstruction of hemiglossectomy defects using the underrated lateral arm free flap with bilobed design.Arch Craniofac Surg. 2019 Feb;20(1):37-43. doi: 10.7181/acfs.2018.02005. Epub 2019 Feb 20. Arch Craniofac Surg. 2019. PMID: 30840817 Free PMC article.
-
Sublingual Lymph Node Metastasis in Early-Stage Floor of the Mouth Carcinoma.Turk Arch Otorhinolaryngol. 2017 Dec;55(4):177-179. doi: 10.5152/tao.2017.2461. Epub 2017 Aug 16. Turk Arch Otorhinolaryngol. 2017. PMID: 29515931 Free PMC article.
-
A Comprehensive Retrospective Institutional Study for Decoding Oral Squamous Cell Carcinoma.Cureus. 2024 Feb 11;16(2):e54001. doi: 10.7759/cureus.54001. eCollection 2024 Feb. Cureus. 2024. PMID: 38476798 Free PMC article.
References
-
- Shah J, Patel SG. Head and Neck Surgery & Oncology. 3rd Edition. Edinburgh: Mosby 2003.
-
- Zbaren P, Nuyens M, Caversaccio M, Stauffer E. Elective neck dissection for carcinomas of the oral cavity: occult metastases, neck recurrences, and adjuvant treatment of pathologically positive necks. Am J Surg 2006;191:756-60. - PubMed
-
- Kaya S, Yilmaz T, Gursel B, Sarac S, Sennaroglu L. The value of elective neck dissection in treatment of cancer of the tongue. Am J Otolaryngol 2001;22:59-64. - PubMed
-
- De Zinis LO, Bolzoni A, Piazza C, Nicolai P. Prevalence and localization of nodal metastases in squamous cell carcinoma of the oral cavity: role and extension of neck dissection. Eur Arch Otorhinolarygol 2006;263:1131-5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical