

Clinical review: Patency of the circuit in continuous renal replacement therapy
- PMID: 17634148
- PMCID: PMC2206533
- DOI: 10.1186/cc5937
Clinical review: Patency of the circuit in continuous renal replacement therapy
Abstract
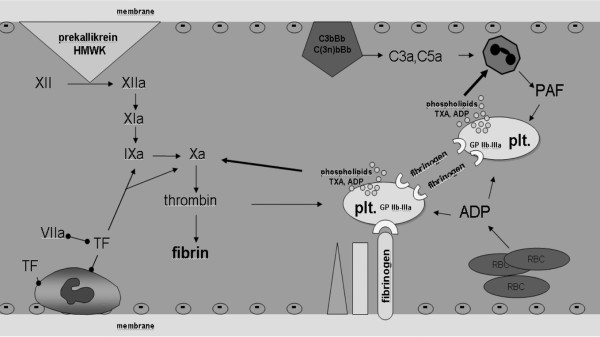
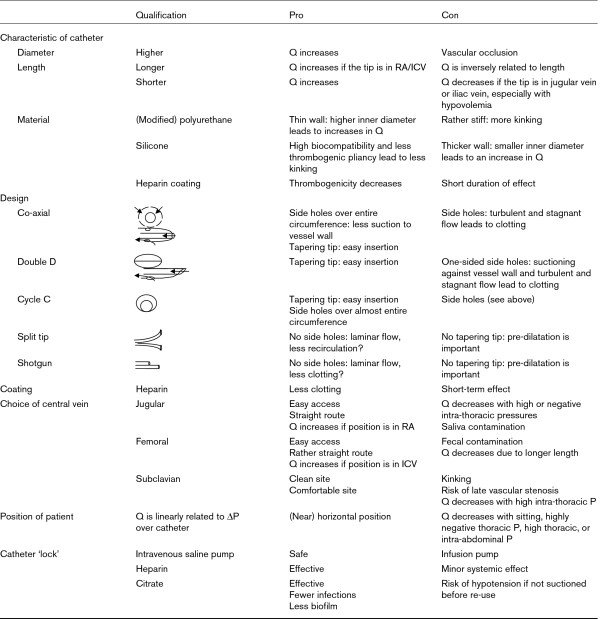
Premature circuit clotting is a major problem in daily practice of continuous renal replacement therapy (CRRT), increasing blood loss, workload, and costs. Early clotting is related to bioincompatibility, critical illness, vascular access, CRRT circuit, and modality. This review discusses non-anticoagulant and anticoagulant measures to prevent circuit failure. These measures include optimization of the catheter (inner diameter, pattern of flow, and position), the settings of CRRT (partial predilution and individualized control of filtration fraction), and the training of nurses. In addition, anticoagulation is generally required. Systemic anticoagulation interferes with plasmatic coagulation, platelet activation, or both and should be kept at a low dose to mitigate bleeding complications. Regional anticoagulation with citrate emerges as the most promising method.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
