

Association of cysteine-rich secretory protein 3 and beta-microseminoprotein with outcome after radical prostatectomy
- PMID: 17634540
- PMCID: PMC2660867
- DOI: 10.1158/1078-0432.CCR-06-3031
Association of cysteine-rich secretory protein 3 and beta-microseminoprotein with outcome after radical prostatectomy
Abstract
Purpose: It has been suggested that cysteine-rich secretory protein 3 (CRISP-3) and beta-microseminoprotein (MSP) are associated with outcome in prostate cancer. We investigated whether these markers are related to biochemical recurrence and whether addition of the markers improves prediction of recurring disease.
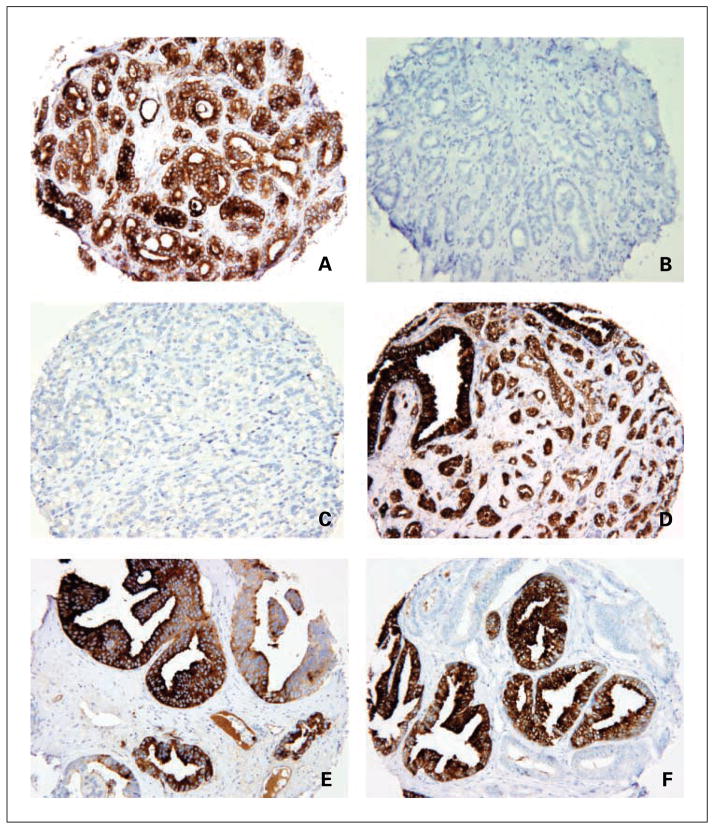
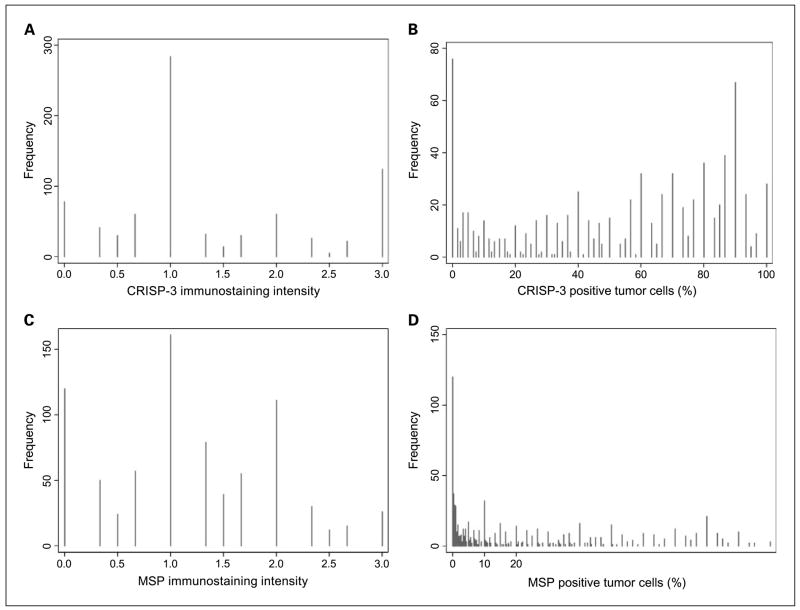
Experimental design: Tissue microarrays of radical prostatectomy specimens were analyzed for CRISP-3 and MSP by immunohistochemistry. Associations between marker positivity and postprostatectomy biochemical recurrence [prostate-specific antigen (PSA) >0.2 ng/mL with a confirmatory level] were evaluated by univariate and multivariable Cox proportional hazards regression. Multivariable analyses controlled for preoperative PSA and pathologic stage and grade.
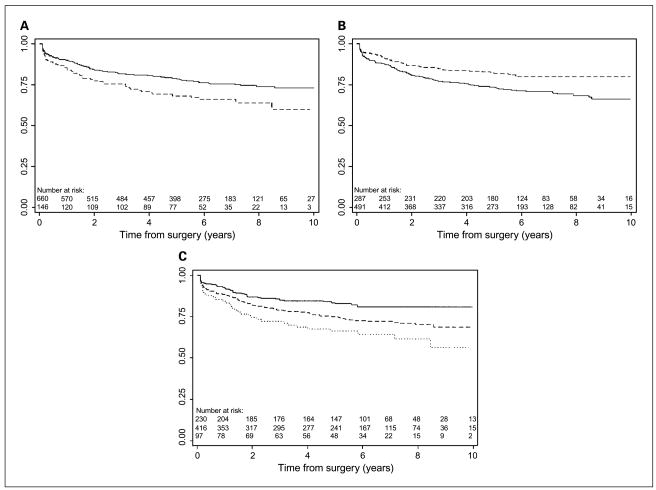
Results: Among 945 patients, 224 had recurrence. Median follow-up for survivors was 6.0 years. Patients positive for CRISP-3 had smaller recurrence-free probabilities, whereas MSP-positive patients had larger recurrence-free probabilities. On univariate analysis, the hazard ratio for patients positive versus negative for CRISP-3 was 1.53 (P=0.010) and for MSP was 0.63 (P=0.004). On multivariable analysis, both CRISP-3 (P=0.007) and MSP (P=0.002) were associated with recurrence. The hazard ratio among CRISP-3-positive/MSP-negative patients compared with CRISP-3-negative/MSP-positive patients was 2.38. Adding CRISP-3 to a base model that included PSA and pathologic stage and grade did not enhance the prediction of recurrence, but adding MSP increased the concordance index minimally from 0.778 to 0.781.
Conclusion: We report evidence that CRISP-3 and MSP are independent predictors of recurrence after radical prostatectomy for localized prostate cancer. However, addition of the markers does not importantly improve the performance of existing predictive models. Further research should aim to elucidate the functions of CRISP-3 and MSP in prostate cancer cells.
Figures
Similar articles
-
Cysteine-rich secretory protein 3 and β-microseminoprotein on prostate cancer needle biopsies do not have predictive value for subsequent prostatectomy outcome.BJU Int. 2011 Oct;108(8):1356-62. doi: 10.1111/j.1464-410X.2010.10059.x. Epub 2011 Mar 16. BJU Int. 2011. PMID: 21410630
-
beta-Microseminoprotein binds CRISP-3 in human seminal plasma.Biochem Biophys Res Commun. 2005 Jul 29;333(2):555-61. doi: 10.1016/j.bbrc.2005.05.139. Biochem Biophys Res Commun. 2005. PMID: 15950934 Free PMC article.
-
Immunohistochemical detection of cysteine-rich secretory protein 3 in tissue and in serum from men with cancer or benign enlargement of the prostate gland.Prostate. 2006 May 1;66(6):591-603. doi: 10.1002/pros.20342. Prostate. 2006. PMID: 16388501
-
Evaluation of the prognostic significance of MSMB and CRISP3 in prostate cancer using automated image analysis.Mod Pathol. 2011 May;24(5):708-19. doi: 10.1038/modpathol.2010.238. Epub 2011 Jan 14. Mod Pathol. 2011. PMID: 21240253
-
The potential value of microseminoprotein-beta as a prostate cancer biomarker and therapeutic target.Prostate. 2010 Feb 15;70(3):333-40. doi: 10.1002/pros.21059. Prostate. 2010. PMID: 19790236 Review.
Cited by
-
The present and future of prostate cancer urine biomarkers.Int J Mol Sci. 2013 Jun 17;14(6):12620-49. doi: 10.3390/ijms140612620. Int J Mol Sci. 2013. PMID: 23774836 Free PMC article. Review.
-
Cysteine-rich secretory protein 3 plays a role in prostate cancer cell invasion and affects expression of PSA and ANXA1.Mol Cell Biochem. 2016 Jan;411(1-2):11-21. doi: 10.1007/s11010-015-2564-2. Epub 2015 Sep 14. Mol Cell Biochem. 2016. PMID: 26369530
-
Screening differentially expressed proteins of coronary heart disease with congenital cold syndrome based on tandem mass tag (TMT) technology.Bioengineered. 2021 Dec;12(1):1338-1350. doi: 10.1080/21655979.2021.1912546. Bioengineered. 2021. PMID: 33904367 Free PMC article.
-
Cysteine- rich secretory protein 3 (CRISP3), ERG and PTEN define a molecular subtype of prostate cancer with implication to patients' prognosis.J Hematol Oncol. 2014 Mar 7;7:21. doi: 10.1186/1756-8722-7-21. J Hematol Oncol. 2014. PMID: 24606912 Free PMC article.
-
Best of the 2007 AUA Annual Meeting: Highlights from the 2007 Annual Meeting of the American Urological Association, May 19-24, 2007, Anaheim, CA.Rev Urol. 2007 Summer;9(3):133-54. Rev Urol. 2007. PMID: 17934570 Free PMC article. No abstract available.
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2006. CA Cancer J Clin. 2006;56:106–30. - PubMed
-
- Kattan MW, Scardino PT, Eastham JA, Stapleton AM, Wheeler TM. A preoperative nomogram for disease recurrence following radical prostatectomy for prostate cancer. J Natl Cancer Inst. 1998;90:766–71. - PubMed
-
- Kattan MW, Wheeler TM, Scardino PT. Postoperative nomogram for disease recurrence after radical prostatectomy for prostate cancer. J Clin Oncol. 1999;17:1499–507. - PubMed
-
- Graefen M, Karakiewicz PI, Cagiannos I, et al. Validation study of the accuracy of a postoperative nomogram for recurrence after radical prostatectomy for localized prostate cancer. J Clin Oncol. 2002;20:951–6. - PubMed
-
- Graefen M, Karakiewicz PI, Cagiannos I, et al. International validation of a preoperative nomogram for prostate cancer recurrence after radical prostatectomy. J Clin Oncol. 2002;20:3206–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
