

Intravenous hypertonic NaCl acts via cerebral sodium-sensitive and angiotensinergic mechanisms to improve cardiac function in haemorrhaged conscious sheep
- PMID: 17640936
- PMCID: PMC2277202
- DOI: 10.1113/jphysiol.2007.139592
Intravenous hypertonic NaCl acts via cerebral sodium-sensitive and angiotensinergic mechanisms to improve cardiac function in haemorrhaged conscious sheep
Abstract
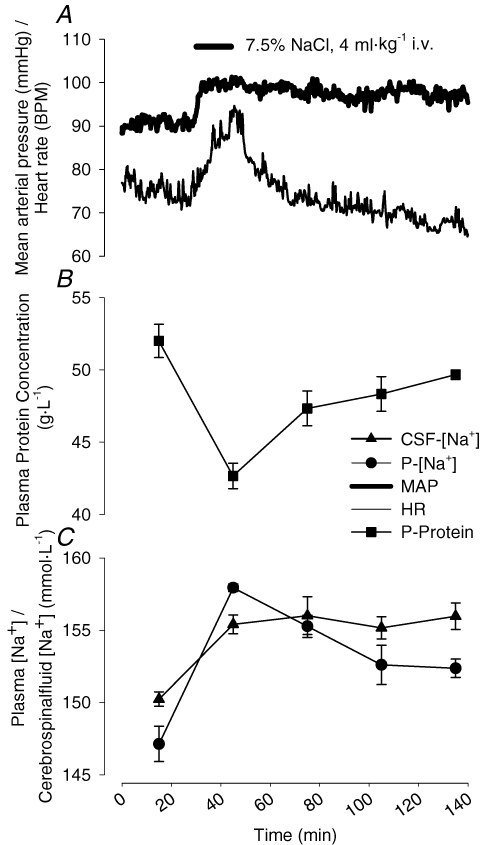
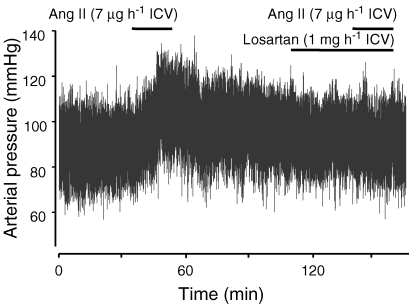
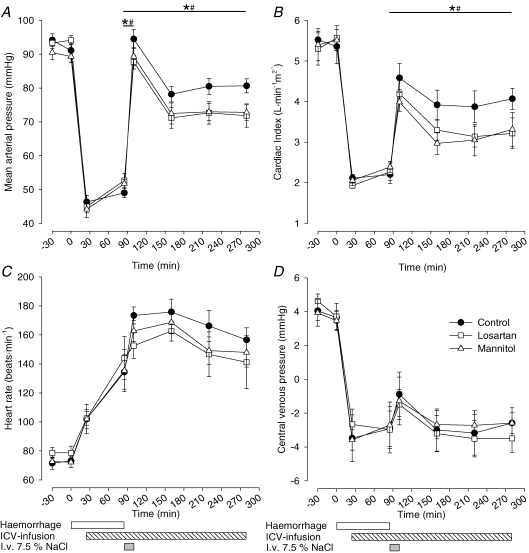
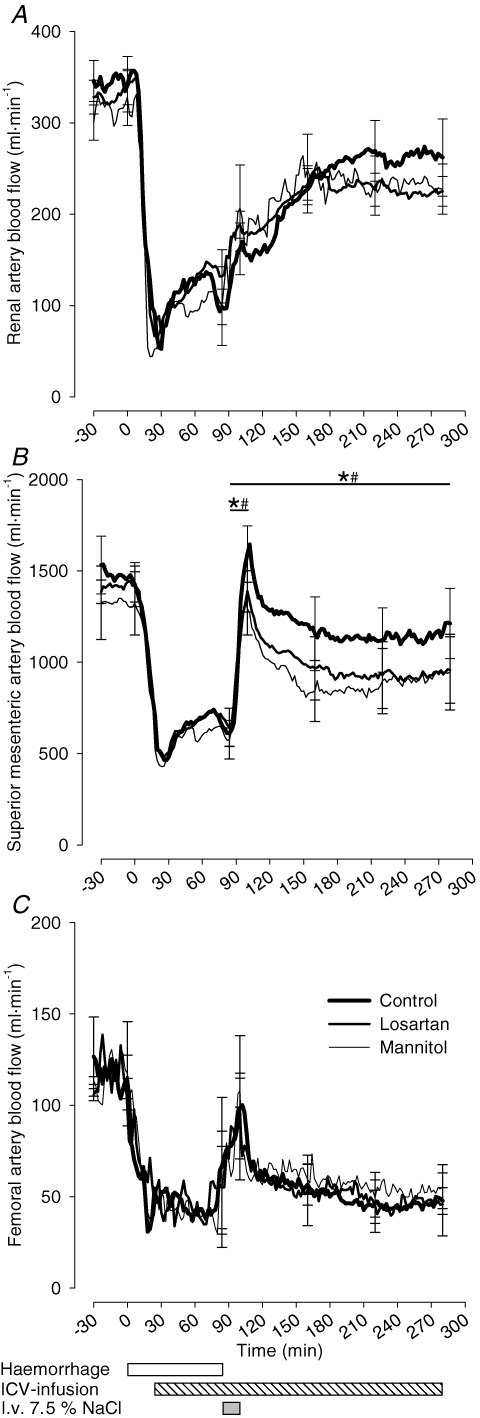
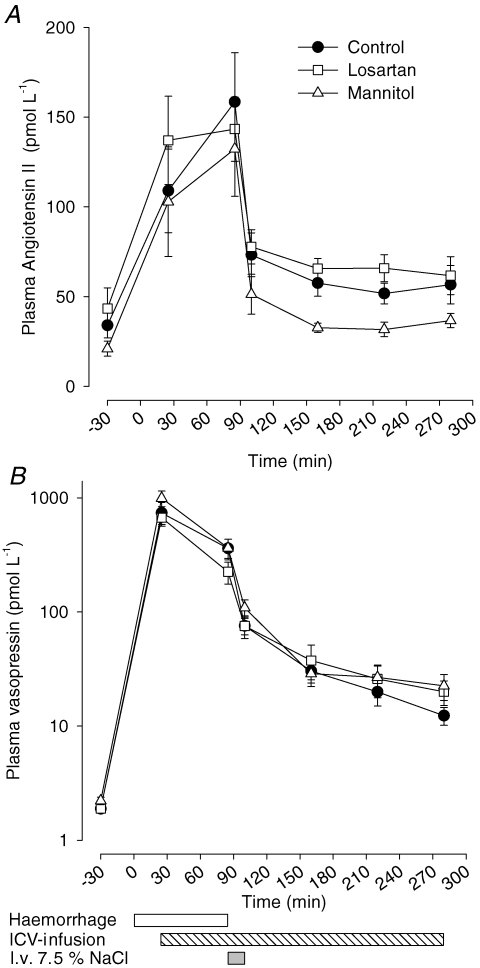
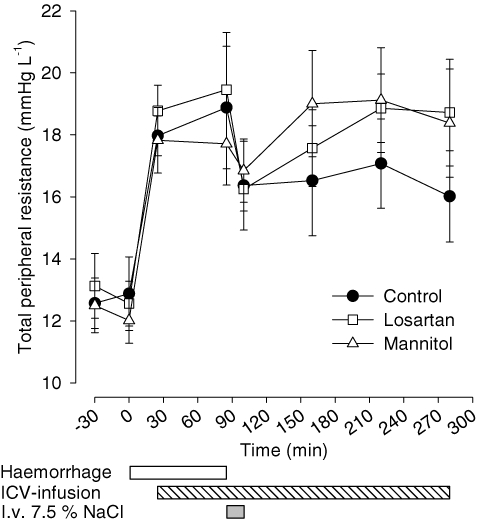
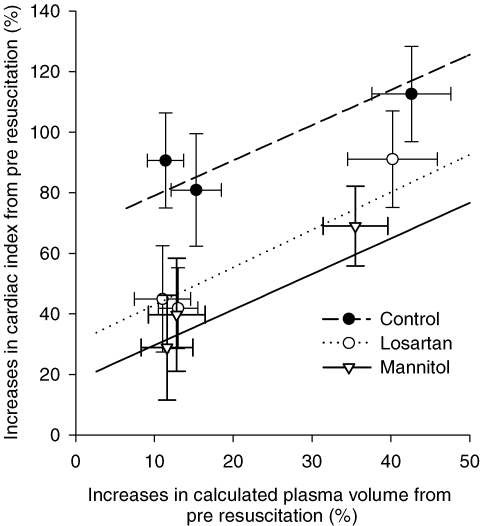
Acute NaCl loading as resuscitation in haemorrhagic hypovolaemia is known to induce rapid cardiovascular recovery. Besides an osmotically induced increase in plasma volume the physiological mechanisms of action are unknown. We hypothesized that a CNS mechanism, elicited by increased periventricular [Na(+)] and mediated by angiotensin II type 1 receptors (AT(1)), is obligatory for the full effect of hypertonic NaCl. To test this we investigated the cardiovascular responses to haemorrhage and subsequent hypertonic NaCl infusion (7.5% NaCl, 4 ml (kg BW)(-1)) in six conscious sheep subjected to intracerebroventricular (i.c.v.) infusion of artificial cerebrospinal fluid (aCSF; control), mannitol solution (Man; 75 mmol l(-1) [Na(+)], total osmolality 295 mosmol kg(-1)) or losartan (Los; 1 mg ml(-1), AT(1) receptor antagonist) at three different occasions. Man normalized (144 +/- 6 mmol l(-1), mean +/- s.d.) the increase in i.c.v. [Na(+)] seen after aCSF (161 +/- 2 mmol l(-1)). Compared with control, both Man and Los significantly (P < 0.05) attenuated the improvement in mean arterial blood pressure (MAP), cardiac index and mesenteric blood flow (SMBF) in response to intravenous hypertonic NaCl: MAP, rapid response +45 mmHg versus +38 mmHg (Man) and +35 mmHg (Los); after 180 min, +32 mmHg versus +21 mmHg (Man) and +19 mmHg (Los); cardiac index after 180 min, +1.9 l min(-1) (m(2))(-1) versus +0.9 l min(-1) (m(2))(-1) (Man) and +0.9 l min(-1) (m(2))(-1) (Los); SMBF rapid response, +981 ml min(-1) versus +719 ml min(-1) (Man) and +744 ml min(-1) (Los); after 180 min, +602 ml min(-1) versus +372 ml min(-1) (Man) and +314 ml min(-1) (Los). The results suggest that increased periventricular [Na(+)] and cerebral AT(1) receptors contribute, together with plasma volume expansion, to improve systemic haemodynamics after treatment with hypertonic NaCl in haemorrhagic hypovolaemia.
Figures
References
-
- Andersson B, Eriksson L, Fernandez O, Kolmodin CG, Oltner R. Centrally mediated effects of sodium and angiotensin II on arterial blood pressure and fluid balance. Acta Physiol Scand. 1972;85:398–407. - PubMed
-
- Andersson B, Jobin M, Olsson K. A study of thirst and other effects of an increased sodium concentration in the 3rd brain ventricle. Acta Physiol Scand. 1967;69:29–36. - PubMed
-
- Barbosa SP, Camargo LA, Saad WA, Renzi A, Luca Junior LA, Menani JV. Lesion of the anteroventral third ventricle region impairs the recovery of arterial pressure induced by hypertonic saline in rats submitted to hemorrhagic shock. Brain Res. 1992;587:109–114. - PubMed
-
- Blair-West JR, Burns P, Denton DA, Ferraro T, McBurnie MI, Tarjan E, Weisinger RS. Thirst induced by increasing brain sodium concentration is mediated by brain angiotensin. Brain Res. 1994;637:335–338. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous