

Contemporary trends in low risk prostate cancer: risk assessment and treatment
- PMID: 17644125
- PMCID: PMC2987559
- DOI: 10.1016/j.juro.2007.03.135
Contemporary trends in low risk prostate cancer: risk assessment and treatment
Abstract
Purpose: We updated national risk trends in prostate cancer with a focus on low risk tumors, reexamined trends in primary treatment for low risk tumors and substratified patients at low risk based on pretreatment clinical data.
Materials and methods: Data were abstracted from the CaPSURE registry. A total of 10,385 men were diagnosed between 1990 and 2006 with localized disease. Low risk was defined as prostate specific antigen 10 ng/ml or less, Gleason score 6 or less and clinical T stage 2a or less. Temporal trends were assessed for patient distribution among risk groups and in the low risk group for individual risk factors, Kattan nomogram prediction, Cancer of the Prostate Risk Assessment score and primary treatment. The ability of the Cancer of the Prostate Risk Assessment score to substratify low risk prostatectomy cases was evaluated with survival analysis.
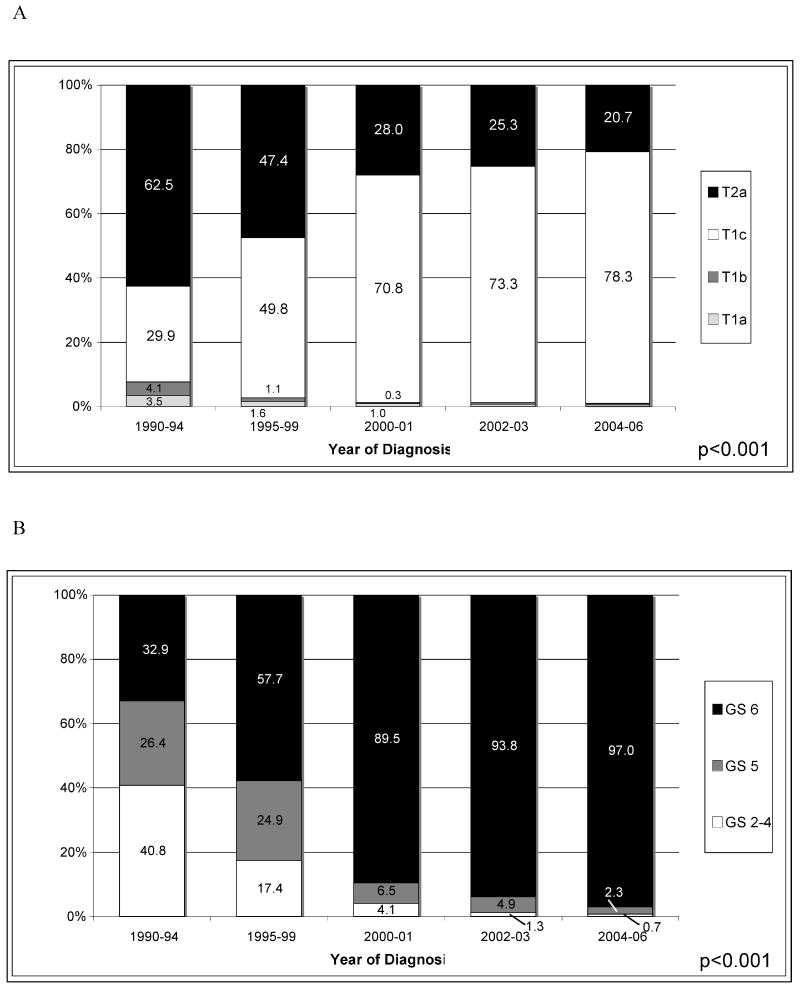
Results: The proportion of low risk tumors in CaPSURE almost doubled from 27.5% in 1990 to 1994, to 46.4% in 2000 to 2001 but it has been relatively constant since then. A growing proportion of low risk tumors are cT1c and virtually all are Gleason score 6. Prostate specific antigen and the percent of positive biopsies decreased throughout the study period, as did the mean Cancer of the Prostate Risk Assessment score. The use of active surveillance increased from a nadir of 6.2% in 2000 to 2001, to 10.2% in 2004 to 2006. The use of prostatectomy also increased, whereas the use of androgen deprivation and radiation decreased. The likelihood of recurrence increased significantly with increasing Cancer of the Prostate Risk Assessment scores.
Conclusions: Patients at low risk can be further substratified to identify those at very low risk based on clinical variables. The use of surveillance is increasing but overtreatment remains a concern in these patients.
Figures



References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43. - PubMed
-
- Bill-Axelson A, Holmberg L, Ruutu M, Haggman M, Andersson SO, Bratell S, et al. Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med. 2005;352:1977. - PubMed
-
- Wei JT, Dunn RL, Sandler HM, McLaughlin PW, Montie JE, Litwin MS, et al. Comprehensive comparison of health-related quality of life after contemporary therapies for localized prostate cancer. J Clin Oncol. 2002;20:557. - PubMed
-
- Roehl KA, Han M, Ramos CG, Antenor JA, Catalona WJ. Cancer progression and survival rates following anatomical radical retropubic prostatectomy in 3,478 consecutive patients: long-term results. J Urol. 2004;172:910. - PubMed
-
- Albertsen PC, Hanley JA, Fine J. 20-year outcomes following conservative management of clinically localized prostate cancer. JAMA. 2005;293:2095. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
