

The cost-effectiveness of four treatments for marijuana dependence
- PMID: 17645430
- PMCID: PMC2398724
- DOI: 10.1111/j.1360-0443.2007.01909.x
The cost-effectiveness of four treatments for marijuana dependence
Abstract
Aim: To analyze data from a randomized clinical trial to determine the cost-effectiveness of using contingency management (CM) and motivational/skills building therapy (motivational enhancement therapy/cognitive-behavioral therapy: MET/CBT) to treat young adults with marijuana dependence. PARTICIPANTS, DESIGN AND MEASUREMENTS: A total of 136 marijuana-dependent young adults, all referred by the criminal justice system, were randomized to one of four treatment conditions: MET/CBT with CM, MET/CBT without CM, drug counseling (DC) with CM and DC without CM. Patient outcome measures include the longest duration of confirmed marijuana abstinence (LDA) during treatment and the total number of marijuana-free urine specimens provided during treatment. Costs were collected retrospectively from the provider and include the costs of therapy, patient drug testing, and those associated with the incentives component (value of vouchers, time to administer the voucher system).
Setting: Out-patient substance abuse clinic in New Haven, Connecticut, USA.
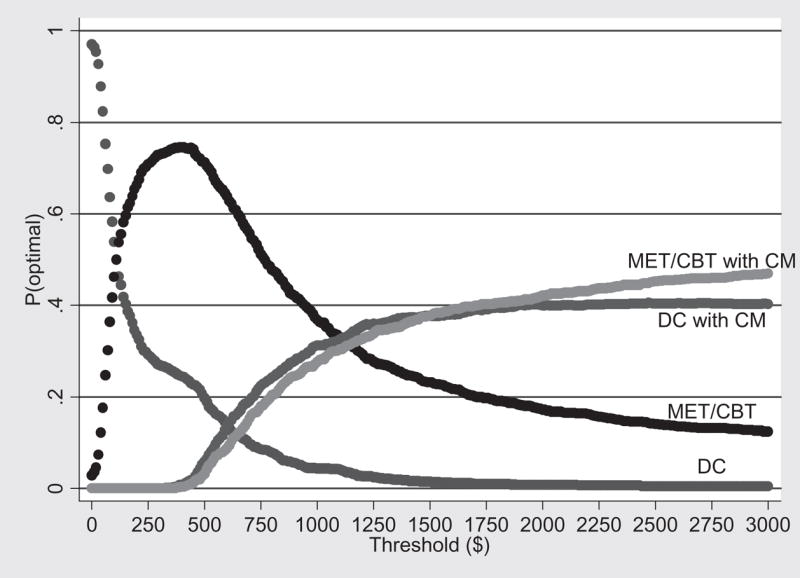
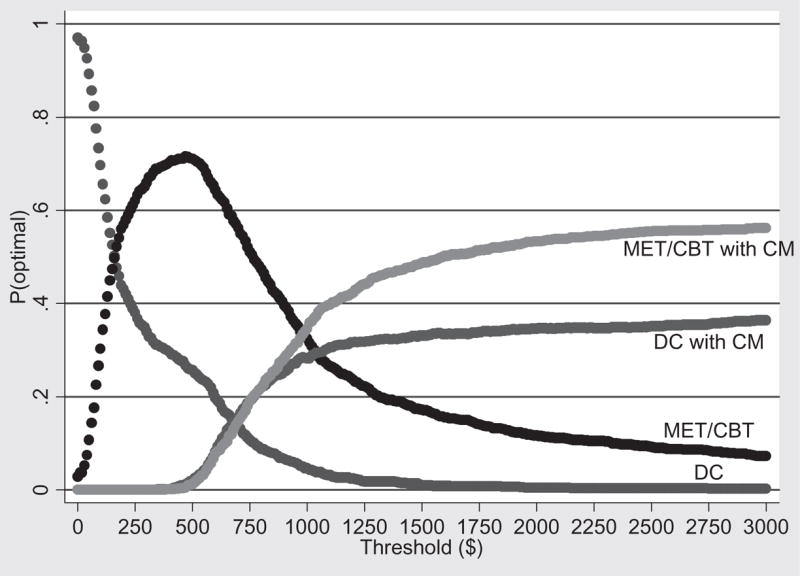
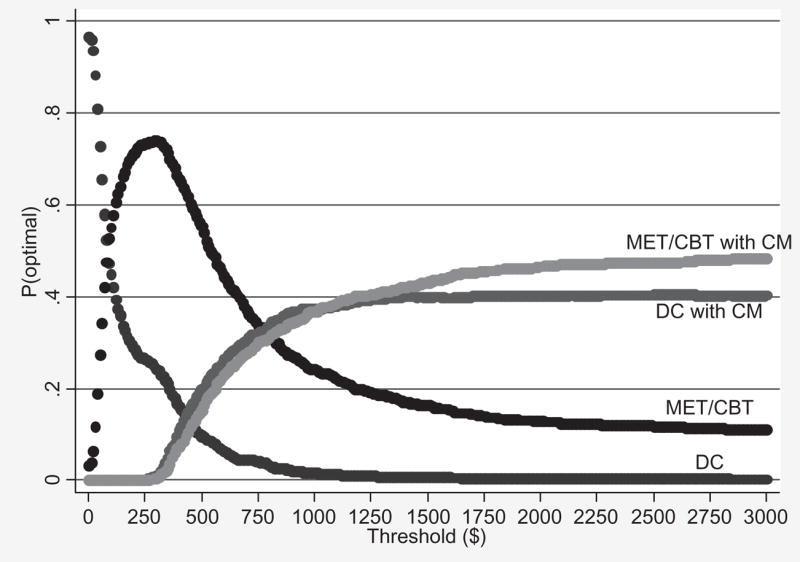
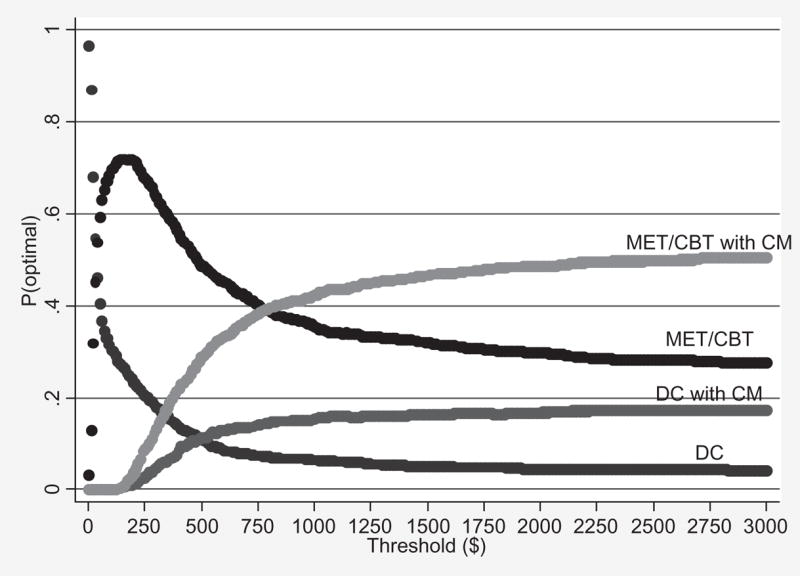
Findings: Which treatment is the most cost-effective depends on the threshold values of an additional week of LDA or an additional marijuana-free urine specimen. For example, the most effective treatment, MET/CBT with CM, was also the most cost-effective treatment at the highest threshold values, while the least effective treatment, DC, was the most cost-effective at the lowest values. Because consensus threshold values for these patient outcomes do not exist, results are presented showing the ranges of values over which each treatment would be considered cost-effective compared to the others. Acceptability curves are presented to show the decision uncertainty associated with these ranges. The results are shown to be robust to (i) sensitivity analyses on several key cost parameters and (ii) patient outcomes measured during the 6-month follow-up period.
Conclusions: This study uses incremental cost-effectiveness ratios and acceptability curves to shed light on the relative cost-effectiveness of four interventions for treating young adults with marijuana dependence. Given the relatively small and specialized nature of our study sample, and the fact that we examined a CM procedure with a single reinforcement schedule, additional studies are warranted to determine the reliability and generalizability of our results both to alternative marijuana-using populations and to CM procedures with alternative incentive parameters. Nevertheless, the relative durability of effects of MET/CBT compared to DC through the 6-month follow-up, and its cost-effectiveness over a comparatively wide range of threshold values, underscores the promise of this approach.
Figures
References
-
- Substance Abuse and Mental Health Services Administration. Results from the 2004 National Survey on Drug Use and Health: National Findings (Office of Applied Studies, NSDUH Series H-28, DHHS Publication No. SMA 05-4062) Rockville, MD: US Department of Health and Human Services; 2005.
-
- Ellickson PL, Martino SC, Collins RL. Marijuana use from adolescence to young adulthood: multiple developmental trajectories and their associated outcomes. Health Psychol. 2004;23:299–307. - PubMed
-
- Windle M, Wiesner M. Trajectories of marijuana use from adolescence to young adulthood: predictors and outcomes. Dev Psychopathol. 2004;16:1007–27. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
