

Predictors of 30-day mortality among patients with Pseudomonas aeruginosa bloodstream infections: impact of delayed appropriate antibiotic selection
- PMID: 17646415
- PMCID: PMC2043259
- DOI: 10.1128/AAC.00338-07
Predictors of 30-day mortality among patients with Pseudomonas aeruginosa bloodstream infections: impact of delayed appropriate antibiotic selection
Abstract
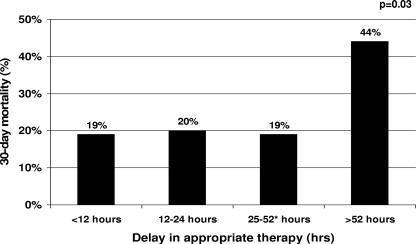
Although a growing number of studies have found a relationship between delayed appropriate antibiotic therapy and mortality, few have attempted to quantify the temporal association between delayed appropriate antibiotic therapy and mortality. This study was designed to measure the elapsed time associated with an increased risk of 30-day mortality among patients with Pseudomonas aeruginosa bacteremia. The retrospective cohort study was conducted among immunocompetent, adult patients with P. aeruginosa bacteremia onset at least 2 days after hospital admission between 1 January 2001 and 30 September 2006. Classification and regression tree analysis (CART) was used to identify the delay in appropriate antibiotic therapy that was associated with an increased risk of 30-day mortality. During the study period, 100 patients met the inclusion criteria. The CART-derived breakpoint between early and delayed treatment was 52 h. The delayed treatment group experienced a >2-fold significant increase in 30-day mortality compared to the early treatment group (44 and 19%, respectively, P = 0.008). Delayed appropriate therapy of >52 h (odds ratio [OR] = 4.1; 95% confidence interval [CI] 1.2 to 13.9, P = 0.03) was independently associated with 30-day mortality in the multivariate analysis. Antibiotic resistance > or =3 classes (adjusted OR [AOR] = 4.6; 95% CI = 1.9 to 11.2, P = 0.001) and chronic obstructive pulmonary disease (AOR = 5.4; 95% CI = 1.5 to 19.7, P = 0.01) were independently associated with delayed appropriate therapy of >52 h. The data strongly suggest that delaying appropriate therapy for approximately 2 days significantly increases the risk of 30-day mortality in patients with P. aeruginosa bloodstream infections.
Figures
References
-
- Bodey, G. P., L. Jadeja, and L. Elting. 1985. Pseudomonas bacteremia: retrospective analysis of 410 episodes. Arch. Intern. Med. 145:1621-1629. - PubMed
-
- Clinical Laboratory Standards Institute. 2006. Performance standards for antimicrobial disk susceptibility tests. Approved standard M2-M9, 9th ed. Clinical Laboratory Standards Institute, Wayne, PA.
-
- Garner, J. S., W. R. Jarvis, T. G. Emori, T. C. Horan, and J. M. Hughes. 1988. CDC definitions for nosocomial infections, 1988. Am. J. Infect. Control 16:128-140. - PubMed
-
- Harbarth, S., K. Ferriere, S. Hugonnet, B. Ricou, P. Suter, and D. Pittet. 2002. Epidemiology and prognostic determinants of bloodstream infections in surgical intensive care. Arch. Surg. 137:1353-1359. - PubMed
-
- Ibrahim, E. H., G. Sherman, S. Ward, V. J. Fraser, and M. H. Kollef. 2000. The influence of inadequate antimicrobial treatment of bloodstream infections on patient outcomes in the ICU setting. Chest 118:146-155. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
