

Effect of Body Mass Index on pregnancy outcomes in nulliparous women delivering singleton babies
- PMID: 17650297
- PMCID: PMC1940246
- DOI: 10.1186/1471-2458-7-168
Effect of Body Mass Index on pregnancy outcomes in nulliparous women delivering singleton babies
Abstract
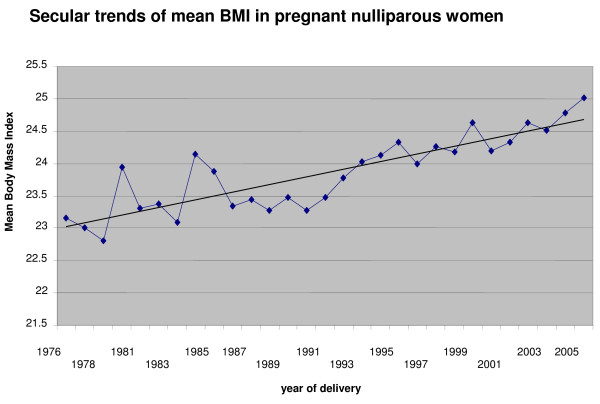
Background: The increasing prevalence of obesity in young women is a major public health concern. These trends have a major impact on pregnancy outcomes in these women, which have been documented by several researchers. In a population based cohort study, using routinely collected data, this paper examines the effect of increasing Body Mass Index (BMI) on pregnancy outcomes in nulliparous women delivering singleton babies.
Methods: This was a retrospective cohort study, based on all nulliparous women delivering singleton babies in Aberdeen between 1976 and 2005. Women were categorized into five groups--underweight (BMI < 20 Kg/m2), normal (BMI 20-24.9 Kg/m2) overweight (BMI 25-29.9 Kg/m2), obese (BMI 30-34.9 Kg/m2) and morbidly obese (BMI > 35 Kg/m2). Obstetric and perinatal outcomes were compared by univariate and multivariate analyses.
Results: In comparison with women of BMI 20-24.9, morbidly obese women faced the highest risk of pre-eclampsia {OR 7.2 (95% CI 4.7, 11.2)} and underweight women the lowest {OR 0.6 (95% CI 0.5, 0.7)}. Induced labour was highest in the morbidly obese {OR 1.8 (95% CI 1.3, 2.5)} and lowest in underweight women {OR 0.8 (95% CI 0.8, 0.9)}. Emergency Caesarean section rates were highest in the morbidly obese {OR 2.8 (95% CI 2.0, 3.9)}, and comparable in women with normal and low BMI. Obese women were more likely to have postpartum haemorrhage {OR 1.5 (95% CI 1.3, 1.7)} and preterm delivery (< 33 weeks) {OR 2.0 (95% CI 1.3, 2.9)}. Birthweights less than 2,500 g were more common in underweight women {OR 1.7 (95% OR 1.2, 2.0)}. The highest risk of birth weights > 4,000 g was in the morbidly obese {OR 2.1 (95% CI 1.3, 3.2)} and the lowest in underweight women {OR 0.5 (95% CI 0.4, 0.6)}.
Conclusion: Increasing BMI is associated with increased incidence of pre-eclampsia, gestational hypertension, macrosomia, induction of labour and caesarean delivery; while underweight women had better pregnancy outcomes than women with normal BMI.
Figures
References
-
- RCOG, 5th October 2006 Press Releases http://www.rcog.org.uk/index.asp?PageID=97&PressReleaseID=126 Accessed 11.12.2006.
-
- Garbaciak JA, Richter MD, Miller S, Barton JJ. Maternal weight and pregnancy complications. Am J Obstet Gynecol. 1985;152:238–245. - PubMed
-
- Abrams BF, Laros RK., Jr Prepregnancy weight, weight gain and body birthweight. Am J Obstet Gynecol. 1986;154:503–509. - PubMed
-
- Naeye RL. Maternal body weight and pregnancy outcome. Am J Clin Nutr. 1990;52:273–279. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
