

How many people have had a myocardial infarction? Prevalence estimated using historical hospital data
- PMID: 17650341
- PMCID: PMC1994682
- DOI: 10.1186/1471-2458-7-174
How many people have had a myocardial infarction? Prevalence estimated using historical hospital data
Abstract
Background: Health administrative data are increasingly used to examine disease occurrence. However, health administrative data are typically available for a limited number of years - posing challenges for estimating disease prevalence and incidence. The objective of this study is to estimate the prevalence of people previously hospitalized with an acute myocardial infarction (AMI) using 17 years of hospital data and to create a registry of people with myocardial infarction.
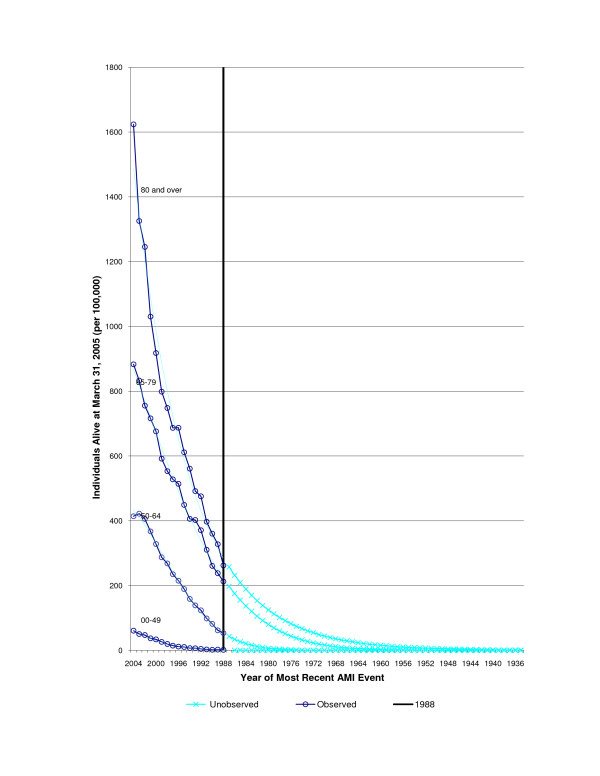
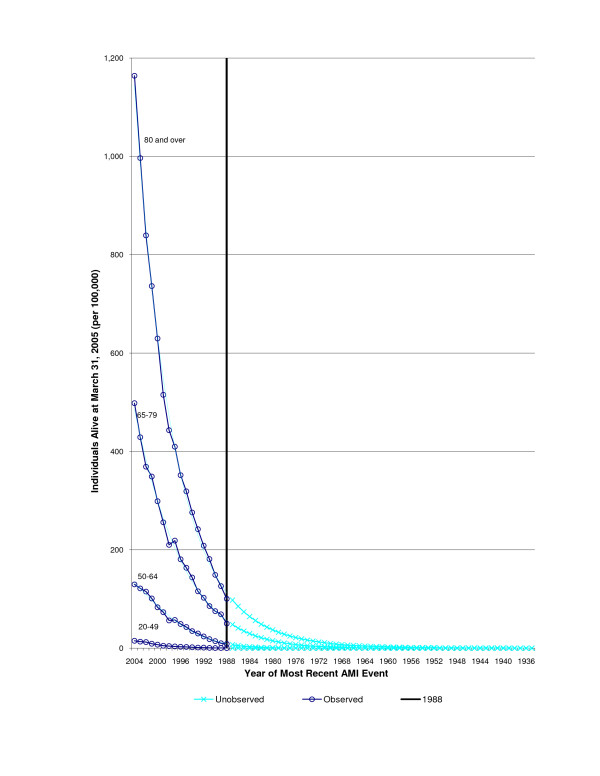
Methods: Myocardial infarction prevalence in Ontario 2004 was estimated using four methods: 1) observed hospital admissions from 1988 to 2004; 2) observed (1988 to 2004) and extrapolated unobserved events (prior to 1988) using a "back tracing" method using Poisson models; 3) DisMod incidence-prevalence-mortality model; 4) self-reported heart disease from the population-based Canadian Community Health Survey (CCHS) in 2000/2001. Individual respondents of the CCHS were individually linked to hospital discharge records to examine the agreement between self-report and hospital AMI admission.
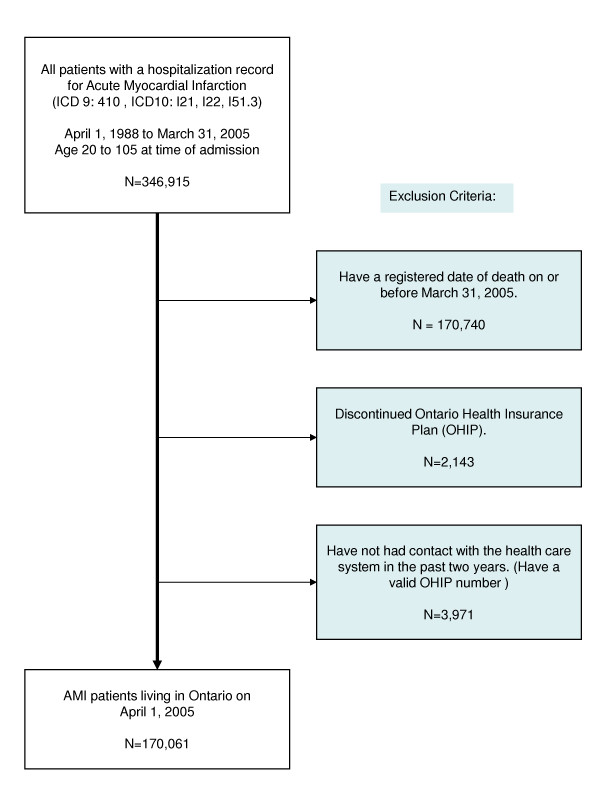
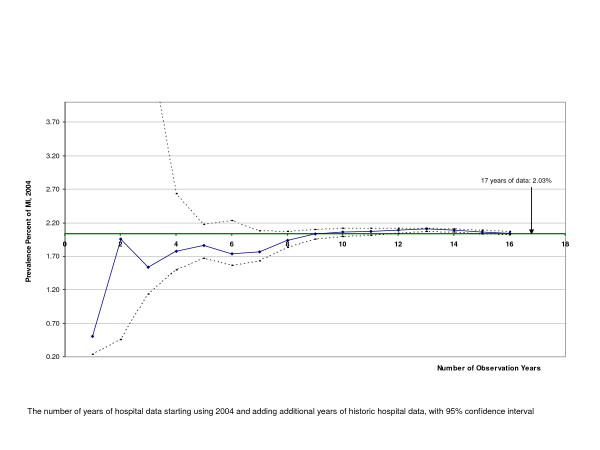
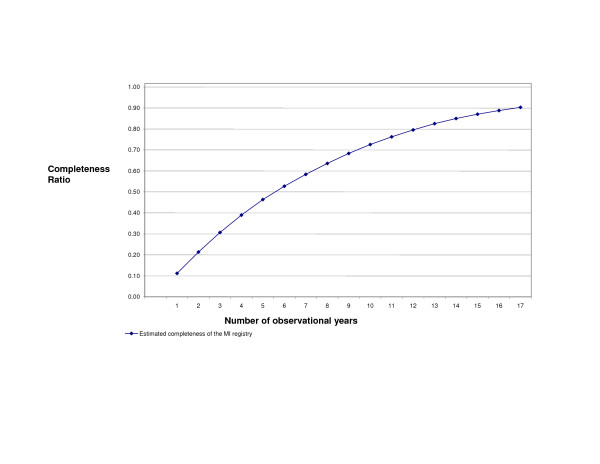
Results: 170,061 Ontario residents who were alive on March 31, 2004, and over age 20 years survived an AMI hospital admission between 1988 to 2004 (cumulative incidence 1.8%). This estimate increased to 2.03% (95% CI 2.01 to 2.05) after adding extrapolated cases that likely occurred before 1988. The estimated prevalence appeared stable with 5 to 10 years of historic hospital data. All 17 years of data were needed to create a reasonably complete registry (90% of estimated prevalent cases). The estimated prevalence using both DisMod and self-reported "heart attack" was higher (2.5% and 2.7% respectively). There was poor agreement between self-reported "heart attack" and the likelihood of having an observed AMI admission (sensitivity = 63.5%, positive predictive value = 54.3%).
Conclusion: Estimating myocardial infarction prevalence using a limited number of years of hospital data is feasible, and validity increases when unobserved events are added to observed events. The "back tracing" method is simple, reliable, and produces a myocardial infarction registry with high estimated "completeness" for jurisdictions with linked hospital data.
Figures
Similar articles
-
Assessing the external validity of model-based estimates of the incidence of heart attack in England: a modelling study.BMC Public Health. 2016 Nov 3;16(1):1135. doi: 10.1186/s12889-016-3782-6. BMC Public Health. 2016. PMID: 27809823 Free PMC article.
-
Temporal analysis of acute myocardial infarction in Ontario, Canada.Can J Cardiol. 2005 Aug;21(10):841-5. Can J Cardiol. 2005. PMID: 16107906
-
[Influence of number of citizens greater than 50 years of age on prevalence of acute myocardial infarction: epidemiological study of Sapporo residents].J Cardiol. 2007 Sep;50(3):167-74. J Cardiol. 2007. PMID: 17941192 Japanese.
-
[Incidence of acute myocardial infarction in Tuscany, 1997-2002: data from the Acute Myocardial Infarction Registry of Tuscany (Tosc-AMI)].Epidemiol Prev. 2006 May-Jun;30(3):161-8. Epidemiol Prev. 2006. PMID: 17051940 Italian.
-
Epidemiology of myocardial infarction in Korea: hospitalization incidence, prevalence, and mortality.Epidemiol Health. 2022;44:e2022057. doi: 10.4178/epih.e2022057. Epub 2022 Jul 12. Epidemiol Health. 2022. PMID: 35843602 Free PMC article. Review.
Cited by
-
Health behaviour changes after diagnosis of chronic illness among Canadians aged 50 or older.Health Rep. 2012 Dec;23(4):49-53. Health Rep. 2012. PMID: 23356045 Free PMC article.
-
Surveillance of ischemic heart disease should include physician billing claims: population-based evidence from administrative health data across seven Canadian provinces.BMC Cardiovasc Disord. 2013 Oct 20;13:88. doi: 10.1186/1471-2261-13-88. BMC Cardiovasc Disord. 2013. PMID: 24138129 Free PMC article.
-
Assessing the external validity of model-based estimates of the incidence of heart attack in England: a modelling study.BMC Public Health. 2016 Nov 3;16(1):1135. doi: 10.1186/s12889-016-3782-6. BMC Public Health. 2016. PMID: 27809823 Free PMC article.
-
Computing disease incidence, prevalence and comorbidity from electronic medical records.J Biomed Inform. 2016 Oct;63:108-111. doi: 10.1016/j.jbi.2016.08.005. Epub 2016 Aug 4. J Biomed Inform. 2016. PMID: 27498067 Free PMC article.
-
Automatic electronic reporting improved the completeness of AMI and stroke incident surveillance in Tianjin, China: a modeling study.Popul Health Metr. 2023 Feb 6;21(1):2. doi: 10.1186/s12963-023-00300-2. Popul Health Metr. 2023. PMID: 36747283 Free PMC article.
References
-
- Clottey C, Mo F, LeBrun B, Mickelson P, Niles J, Robbins G. The development of the National Diabetes Surveillance System (NDSS) in Canada. Chronic Dis Can. 2001;22:67–69. - PubMed
-
- Potter BK, Manuel D, Speechley KN, Gutmanis IA, Campbell MK, Koval JJ. Is there value in using physician billing claims along with other administrative health care data to document the burden of adolescent injury? An exploratory investigation with comparison to self-reports in Ontario, Canada. BMC Health Serv Res. 2005;5:15. doi: 10.1186/1472-6963-5-15. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
