

A comparison of diabetic foot ulcer outcomes using negative pressure wound therapy versus historical standard of care
- PMID: 17651226
- PMCID: PMC7951410
- DOI: 10.1111/j.1742-481X.2007.00317.x
A comparison of diabetic foot ulcer outcomes using negative pressure wound therapy versus historical standard of care
Abstract
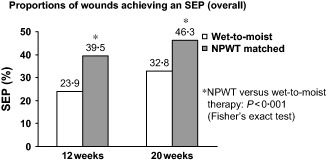
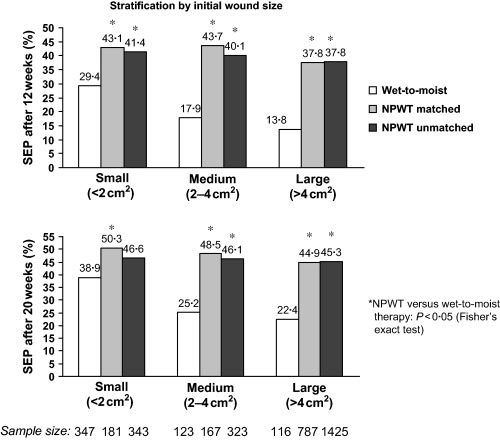
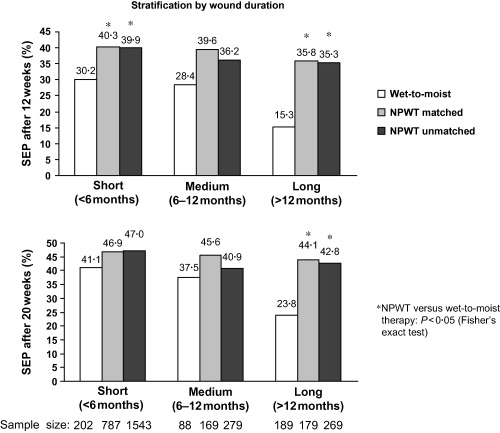
Diabetic foot ulcers (DFUs) are a leading cause of morbidity and hospitalisation among patients with diabetes. We analysed claims data for Medicare part B diabetic foot ulcer patients treated with Negative Pressure Wound Therapy at home (N = 1135) and diabetic foot ulcer patients from a published meta-analysis of randomised controlled wet-to-moist therapy. The expected costs of care for the two treatments were also compared. A significantly greater proportion of wounds treated with NPWT achieved a successful treatment endpoint compared with wet-to-moist therapy at both 12 weeks (39.5% versus 23.9%; P < 0.001) and 20 weeks (46.3% versus 32.8%; P < 0.001). NPWT-treated patients reached a successful wound treatment endpoint more rapidly, and the benefit was apparent in all wound sizes. Expected 20-week treatment costs for NPWT were similar to those for wet-to-moist therapy if one nursing visit per day for the latter is assumed but 42% less if two nursing visits per day are made. Thus, NPWT may improve the proportion of DFUs that attain a successful wound treatment endpoint and decrease resource utilisation by a given health care system compared with standard wet-to-moist therapy.
Figures
References
-
- Ramsey SD, Newton K, Blough D, McCulloch DK, Sandhu N, Reiber GE, Wagner EH. Incidence, outcomes, and cost of foot ulcers in patients with diabetes. Diabetes Care 1999;22:382–7. - PubMed
-
- Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA 2005;293:217–28. - PubMed
-
- American Diabetes Association . Consensus Development Conference on Diabetic Foot Wound Care: 7–8 April 1999, Boston Massachusetts. Diabetes Care 1999;22:1354–60. - PubMed
-
- Larsson J, Agardh CD, Apelqvist J, Stenstrom A. Long‐term prognosis after healed amputation in patients with diabetes. Clin Orthop 1998;350:149–58. - PubMed
-
- Pecoraro RE, Reiber GE, Burgess EM. Pathways to diabetic limb amputation. Basis for prevention. Diabetes Care 1990;13:513–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
