

Vasopressin improves survival in a porcine model of abdominal vascular injury
- PMID: 17659093
- PMCID: PMC2206489
- DOI: 10.1186/cc5977
Vasopressin improves survival in a porcine model of abdominal vascular injury
Abstract
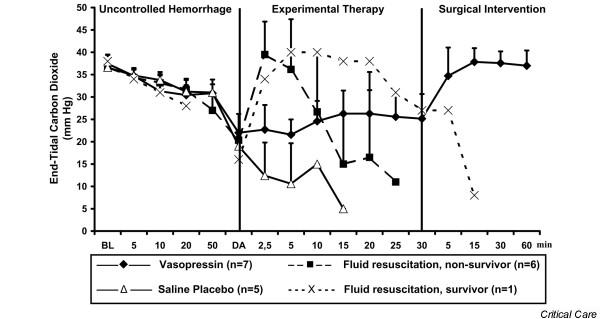
Introduction: We sought to determine and compare the effects of vasopressin, fluid resuscitation and saline placebo on haemodynamic variables and short-term survival in an abdominal vascular injury model with uncontrolled haemorrhagic shock in pigs.
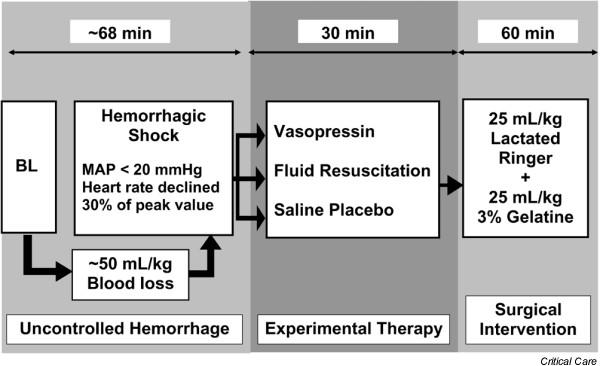
Methods: During general anaesthesia, a midline laparotomy was performed on 19 domestic pigs, followed by an incision (width about 5 cm and depth 0.5 cm) across the mesenterial shaft. When mean arterial blood pressure was below 20 mmHg, and heart rate had declined progressively, experimental therapy was initiated. At that point, animals were randomly assigned to receive vasopressin (0.4 U/kg; n = 7), fluid resuscitation (25 ml/kg lactated Ringer's and 25 ml/kg 3% gelatine solution; n = 7), or a single injection of saline placebo (n = 5). Vasopressin-treated animals were then given a continuous infusion of 0.08 U/kg per min vasopressin, whereas the remaining two groups received saline placebo at an equal rate of infusion. After 30 min of experimental therapy bleeding was controlled by surgical intervention, and further fluid resuscitation was performed. Thereafter, the animals were observed for an additional hour.
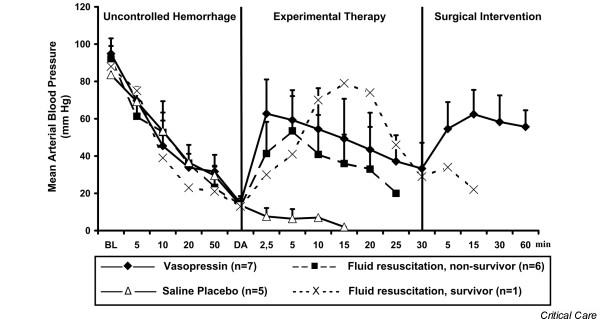
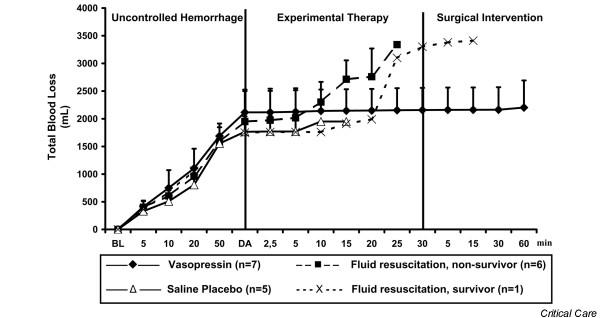
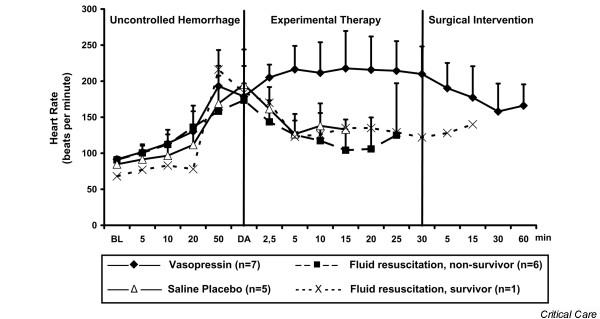
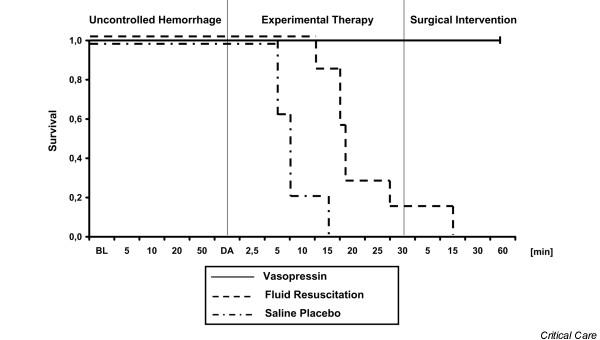
Results: After 68 +/- 19 min (mean +/- standard deviation) of uncontrolled bleeding, experimental therapy was initiated; at that time total blood loss and mean arterial blood pressure were similar between groups (not significant). Mean arterial blood pressure increased in both vasopressin-treated and fluid-resuscitated animals from about 15 mmHg to about 55 mmHg within 5 min, but afterward it decreased more rapidly in the fluid resuscitation group; mean arterial blood pressure in the placebo group never increased. Seven out of seven vasopressin-treated animals survived, whereas six out of seven fluid-resuscitated and five out of five placebo pigs died before surgical intervention was initiated (P < 0.0001).
Conclusion: Vasopressin, but not fluid resuscitation or saline placebo, ensured short-term survival in this vascular injury model with uncontrolled haemorrhagic shock in sedated pigs.
Figures
Similar articles
-
Arginine vasopressin, but not epinephrine, improves survival in uncontrolled hemorrhagic shock after liver trauma in pigs.Crit Care Med. 2003 Apr;31(4):1160-5. doi: 10.1097/01.CCM.0000060014.75282.69. Crit Care Med. 2003. PMID: 12682488
-
Continuous infusion of small-volume fluid resuscitation in the treatment of combined uncontrolled hemorrhagic shock and head injury.J Coll Physicians Surg Pak. 2007 Jan;17(1):19-22. J Coll Physicians Surg Pak. 2007. PMID: 17204214
-
Vasopressin, but not fluid resuscitation, enhances survival in a liver trauma model with uncontrolled and otherwise lethal hemorrhagic shock in pigs.Anesthesiology. 2003 Mar;98(3):699-704. doi: 10.1097/00000542-200303000-00018. Anesthesiology. 2003. PMID: 12606914
-
Developing alternative strategies for the treatment of traumatic haemorrhagic shock.Curr Opin Crit Care. 2008 Jun;14(3):247-53. doi: 10.1097/MCC.0b013e3282fce62a. Curr Opin Crit Care. 2008. PMID: 18467882 Review.
-
Vasopressin in hemorrhagic shock: review article.Am Surg. 2009 Dec;75(12):1207-12. Am Surg. 2009. PMID: 19999914 Review.
Cited by
-
Effects of Vasopressin Receptor Agonists during the Resuscitation of Hemorrhagic Shock: A Systematic Review and Meta-Analysis of Experimental and Clinical Studies.J Pers Med. 2023 Jul 16;13(7):1143. doi: 10.3390/jpm13071143. J Pers Med. 2023. PMID: 37511756 Free PMC article.
-
Does vasopressor therapy have an indication in hemorrhagic shock?Ann Intensive Care. 2013 May 22;3(1):13. doi: 10.1186/2110-5820-3-13. Ann Intensive Care. 2013. PMID: 23697682 Free PMC article.
-
A Rationale for the Use of Norepinephrine after the Control of Bleeding in Hemorrhagic Shock?Am J Respir Crit Care Med. 2022 Jul 1;206(1):1-2. doi: 10.1164/rccm.202203-0521ED. Am J Respir Crit Care Med. 2022. PMID: 35446239 Free PMC article. No abstract available.
-
Vasopressin in hemorrhagic shock: a systematic review and meta-analysis of randomized animal trials.Biomed Res Int. 2014;2014:421291. doi: 10.1155/2014/421291. Epub 2014 Sep 1. Biomed Res Int. 2014. PMID: 25254206 Free PMC article.
-
Modern resuscitation of hemorrhagic shock: what is on the horizon?Eur J Trauma Emerg Surg. 2014 Dec;40(6):641-56. doi: 10.1007/s00068-014-0416-5. Epub 2014 Jun 17. Eur J Trauma Emerg Surg. 2014. PMID: 26814779
References
-
- Kwan I, Bunn F, Roberts I, WHO Pre-Hospital Trauma Care Steering Committee Timing and volume of fluid administration for patients with bleeding. Cochrane Database Syst Rev. 2003;3:CD002245. - PubMed
-
- Voelckel WG, Raedler C, Wenzel V, Lindner KH, Krismer AC, Schmittinger CA, Herff H, Rheinberger K, Königsrainer A. Arginine vasopressin, but not epinephrine, improves survival in uncontrolled hemorrhagic shock after liver trauma in pigs. Crit Care Med. 2003;31:1160–1165. doi: 10.1097/01.CCM.0000060014.75282.69. - DOI - PubMed
-
- Stadlbauer KH, Wagner-Berger HG, Raedler C, Voelckel WG, Wenzel V, Krismer AC, Klima G, Rheinberger K, Nussbaumer W, Pressmar D, et al. Vasopressin, but not fluid resuscitation, enhances survival in a liver trauma model with uncontrolled and otherwise lethal hemorrhagic shock in pigs. Anesthesiology. 2003;98:699–704. doi: 10.1097/00000542-200303000-00018. - DOI - PubMed
-
- Raedler C, Voelckel WG, Wenzel V, Krismer AC, Schmittinger CA, Herff H, Mayr VD, Stadlbauer KH, Lindner KH, Königsrainer A. Treatment of uncontrolled hemorrhagic shock after liver trauma: fatal effects of fluid resuscitation versus improved outcome after vasopressin. Anesth Analg. 2004;98:1759–1766. doi: 10.1213/01.ANE.0000117150.29361.5A. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
