

Metabolic liver disease of obesity and role of adipose tissue in the pathogenesis of nonalcoholic fatty liver disease
- PMID: 17659704
- PMCID: PMC4146793
- DOI: 10.3748/wjg.v13.i26.3540
Metabolic liver disease of obesity and role of adipose tissue in the pathogenesis of nonalcoholic fatty liver disease
Abstract
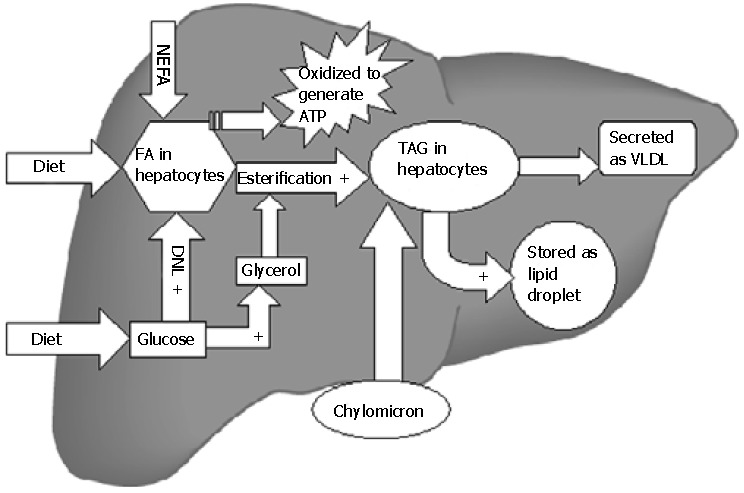
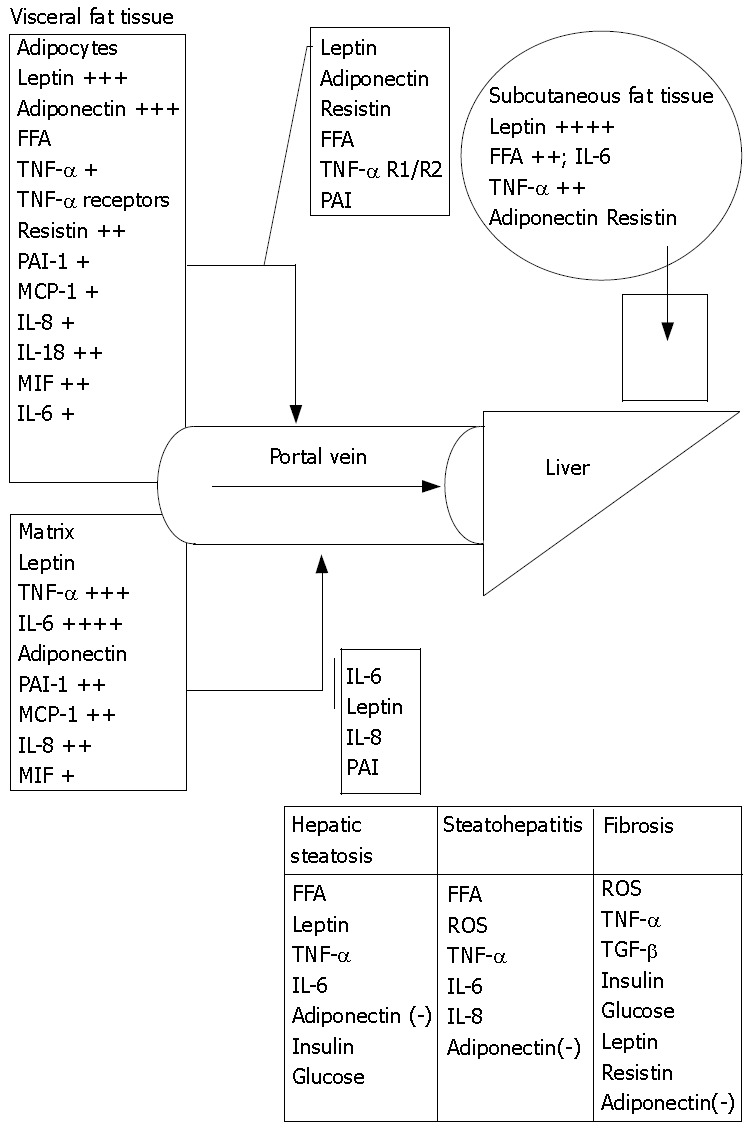
Nonalcoholic fatty liver disease (NAFLD) is an increasingly recognized cause of liver-related morbidity and mortality. It can develop secondary to numerous causes but a great majority of NAFLD cases occur in patients who are obese or present with other components of metabolic syndrome (hypertension, dyslipidemia, diabetes). This is called primary NAFLD and insulin resistance plays a key role in its pathogenesis. Obesity is characterized by expanded adipose tissue, which is under a state of chronic inflammation. This disturbs the normal storage and endocrine functions of adipose tissue. In obesity, the secretome (adipokines, cytokines, free fatty acids and other lipid moieties) of fatty tissue is amplified, which through its autocrine, paracrine actions in fat tissue and systemic effects especially in the liver leads to an altered metabolic state with insulin resistance (IR). IR leads to hyperglycemia and reactive hyperinsulinemia, which stimulates lipid-accumulating processes and impairs hepatic lipid metabolism. IR enhances free fatty acid delivery to liver from the adipose tissue storage due to uninhibited lipolysis. These changes result in hepatic abnormal fat accumulation, which may initiate the hepatic IR and further aggravate the altered metabolic state of whole body. Hepatic steatosis can also be explained by the fact that there is enhanced dietary fat delivery and physical inactivity. IR and NAFLD are also seen in various lipodystrophic states in contrary to popular belief that these problems only occur due to excessive adiposity in obesity. Hence, altered physiology of adipose tissue is central to development of IR, metabolic syndrome and NAFLD.
Figures
Similar articles
-
[Metabolic fatty liver diseases: hepatic consequences of the metabolic syndrome].Gastroenterol Clin Biol. 2007 Dec;31(12):1127-34. doi: 10.1016/s0399-8320(07)78350-1. Gastroenterol Clin Biol. 2007. PMID: 18176372 Review. French.
-
Non-alcoholic fatty liver disease, obesity and the metabolic syndrome.Best Pract Res Clin Gastroenterol. 2014 Aug;28(4):637-53. doi: 10.1016/j.bpg.2014.07.008. Epub 2014 Jul 11. Best Pract Res Clin Gastroenterol. 2014. PMID: 25194181 Review.
-
Effect of adipose tissue insulin resistance on metabolic parameters and liver histology in obese patients with nonalcoholic fatty liver disease.Hepatology. 2012 May;55(5):1389-97. doi: 10.1002/hep.25539. Epub 2012 Mar 18. Hepatology. 2012. PMID: 22183689
-
Crosstalk between adipose tissue insulin resistance and liver macrophages in non-alcoholic fatty liver disease.J Hepatol. 2019 Nov;71(5):1012-1021. doi: 10.1016/j.jhep.2019.06.031. Epub 2019 Jul 10. J Hepatol. 2019. PMID: 31301321
-
Non-alcoholic fatty liver disease and obesity: biochemical, metabolic and clinical presentations.World J Gastroenterol. 2014 Jul 28;20(28):9330-7. doi: 10.3748/wjg.v20.i28.9330. World J Gastroenterol. 2014. PMID: 25071327 Free PMC article. Review.
Cited by
-
Synergistic effect of fatty liver and smoking on metabolic syndrome.World J Gastroenterol. 2009 Nov 14;15(42):5334-9. doi: 10.3748/wjg.15.5334. World J Gastroenterol. 2009. PMID: 19908343 Free PMC article.
-
Early Hepatic Oxidative Stress and Mitochondrial Changes Following Western Diet in Middle Aged Rats.Nutrients. 2019 Nov 5;11(11):2670. doi: 10.3390/nu11112670. Nutrients. 2019. PMID: 31694213 Free PMC article.
-
Isolation, Characterization, and Purification of Macrophages from Tissues Affected by Obesity-related Inflammation.J Vis Exp. 2017 Apr 3;(122):55445. doi: 10.3791/55445. J Vis Exp. 2017. PMID: 28447981 Free PMC article.
-
Atorvastatin and Flaxseed Effects on Biochemical Indices and Hepatic Fat of NAFLD Model in Rats.Adv Biomed Res. 2023 Apr 25;12:98. doi: 10.4103/abr.abr_21_22. eCollection 2023. Adv Biomed Res. 2023. PMID: 37288026 Free PMC article.
-
Anti-Obesity Effects of Sargassum thunbergii via Downregulation of Adipogenesis Gene and Upregulation of Thermogenic Genes in High-Fat Diet-Induced Obese Mice.Nutrients. 2020 Oct 29;12(11):3325. doi: 10.3390/nu12113325. Nutrients. 2020. PMID: 33138053 Free PMC article.
References
-
- Ludwig J, Viggiano TR, McGill DB, Oh BJ. Nonalcoholic steatohepatitis: Mayo Clinic experiences with a hitherto unnamed disease. Mayo Clin Proc. 1980;55:434–438. - PubMed
-
- Clark JM, Brancati FL, Diehl AM. Nonalcoholic fatty liver disease. Gastroenterology. 2002;122:1649–1657. - PubMed
-
- Ruhl CE, Everhart JE. Epidemiology of nonalcoholic fatty liver. Clin Liver Dis. 2004;8:501–519, vii. - PubMed
-
- Farrell GC, Larter CZ. Nonalcoholic fatty liver disease: from steatosis to cirrhosis. Hepatology. 2006;43:S99–S112. - PubMed
-
- Bellentani S, Tiribelli C, Saccoccio G, Sodde M, Fratti N, De Martin C, Cristianini G. Prevalence of chronic liver disease in the general population of northern Italy: the Dionysos Study. Hepatology. 1994;20:1442–1449. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
