

Review
doi: 10.1016/j.semcdb.2007.05.004.
Epub 2007 May 18.
Physiology and electrical activity of uterine contractions
Affiliations
- PMID: 17659954
- PMCID: PMC2048588
- DOI: 10.1016/j.semcdb.2007.05.004
Item in Clipboard
Review
Physiology and electrical activity of uterine contractions
Semin Cell Dev Biol.
2007 Jun.
Abstract
Presently, there is no effective treatment for preterm labor. The most obvious reason for this anomaly is that there is no objective manner to evaluate the progression of pregnancy through steps leading to labor, either at term or preterm. Several techniques have been adopted to monitor labor, and/or to diagnose labor, but they are either subjective or indirect, and they do not provide an accurate prediction of when labor will occur. With no method to determine preterm labor, treatment might never improve. Uterine electromyography (EMG) methods may provide such needed diagnostics.
Figures
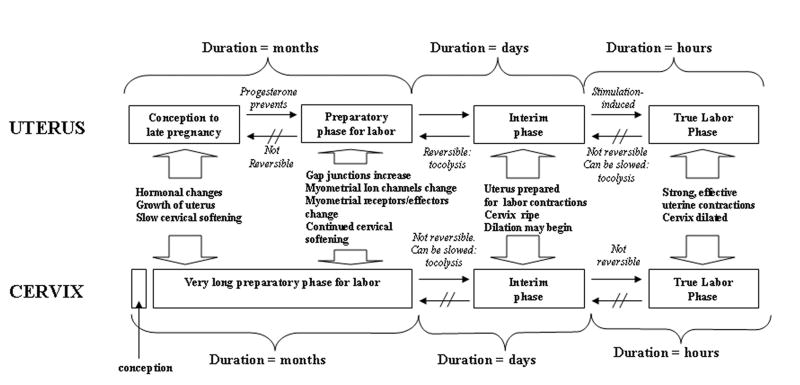
A model of maturation for the uterus and cervix, from conception to delivery. The uterine and cervical steps to normal development occur over different time scales and gestations. However, the interim phase, just prior to dilation and before forceful and effective contractions, might be the final chance to treat most patients who are experiencing initial preterm labor symptoms.
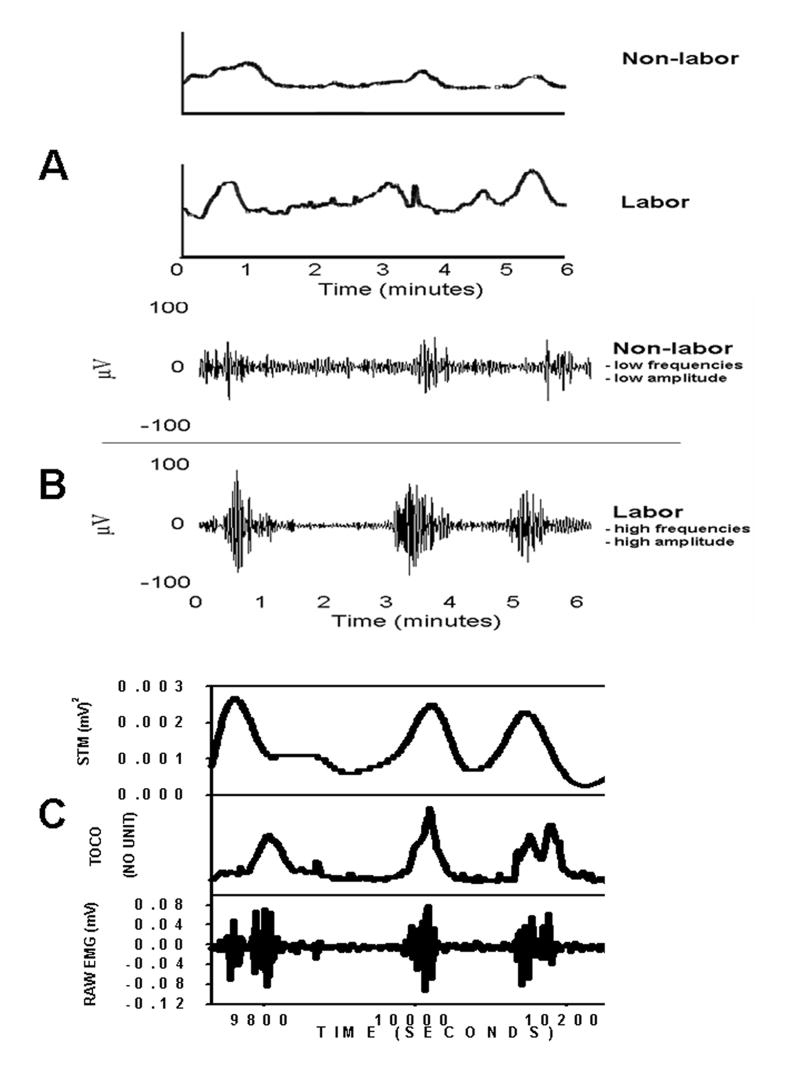
A.) Tocodynamometer (TOCO) recordings from a patient in term labor (bottom trace) and from a term non-labor patient (top trace). Note that the approximate contraction rates, and even some of the amplitudes, are equal. This is problematic for the instrument’s user when using the TOCO device to distinguish between the two patient types. These types of failure often occur when the TOCO device is utilized in the clinic. Nevertheless, clinicians have become accustomed to using them, despite the shortcomings of the instrument. B.) On the other hand, differences clearly manifest themselves (some of which can be discerned visually and some which must be calculated) when comparing the uterine EMG recording of a term labor patient (bottom trace) to a term non-labor patient (top trace). Labor patient uterine EMG’s generally possesses higher burst amplitudes and higher action potential frequencies within each burst than those of non-labor patients. C.) In the future, real-time raw EMG signals (bottom trace) could be converted to “TOCO-like” signals (top – trace; using spectral temporal mapping – STM – for example) to facilitate the ease of translation by physicians in the clinic. Compare this to the irregular and difficult-to-interpret trace (middle trace) produced simultaneously by the TOCO on the same patient.
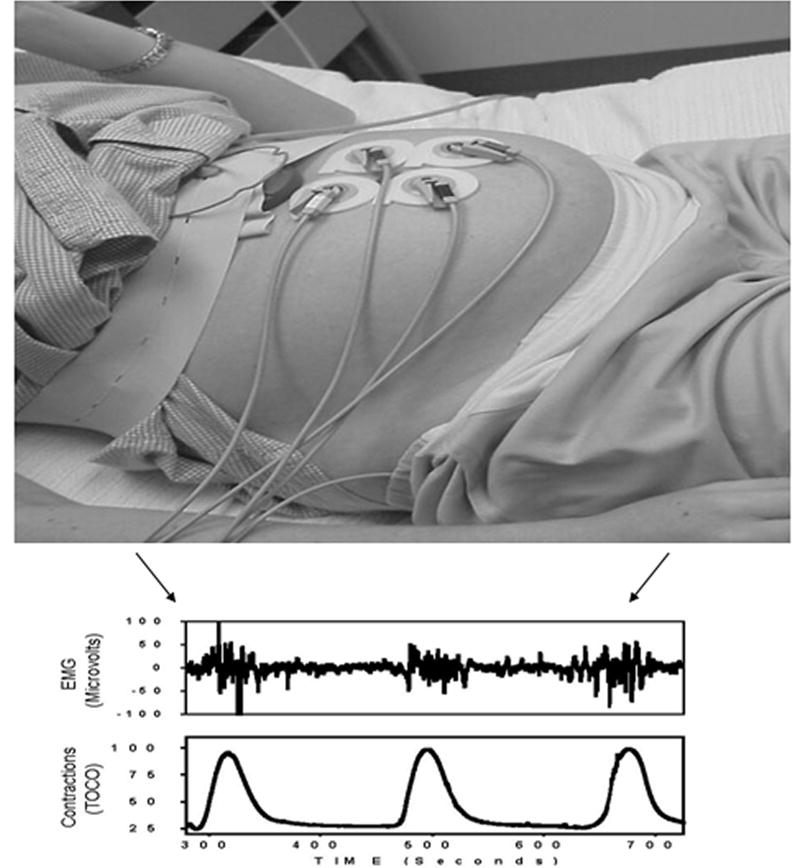
Typical uterine EMG setup includes abdominal surface electrodes, electrical filters/amplifiers and acquisition and analysis hardware/software. The EMG bursts that are responsible for uterine contractions are shown in clear temporal correspondence with the simultaneous TOCO output. However, the TOCO can only measure contraction rate and (crudely and inaccurately) contraction amplitude. The uterine EMG signals, on the other hand, can be analyzed by a number of sophisticated mathematical methods (power spectrum, wavelets, fractals, and artificial neural networks to name a few) in order to determine the extent of electrochemical preparedness of the myometrium for labor and subsequent delivery.
References
-
- US Preventive Services Task Force. Guide to Clinical Preventive Services: An Assessment of the Effectiveness of 169 Interventions. Baltimore, MD: Williams & Wilkins; 1989.
-
- Brown ER, Epstein M. Immediate consequences of preterm birth. In: Fuchs F, Stubblefield PG, editors. Preterm birth: causes, prevention, and management. New York: Macmillan Publishing; 1984. p. 323.
-
- Brown ER. Long-term sequelae of preterm birth. In: Fuchs F, Stubblefield PG, editors. Preterm birth: causes, prevention, and management. New York: Macmillan Publishing; 1984. p. 333.
-
- Kao CY. Electrical properties of uterine smooth muscle. In: Wynn RM, editor. Biology of the Uterus. Plenum Press; New York: 1977. pp. 423–496.
-
- Marshall JM. Regulation of activity in uterine smooth muscle. Physiol Rev. 1962;42:213–227. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
