

National failure to operate on early stage pancreatic cancer
- PMID: 17667493
- PMCID: PMC1933550
- DOI: 10.1097/SLA.0b013e3180691579
National failure to operate on early stage pancreatic cancer
Abstract
Background: Despite studies demonstrating improved outcomes, pessimism persists regarding the effectiveness of surgery for pancreatic cancer. Our objective was to evaluate utilization of surgery in early stage disease and identify factors predicting failure to undergo surgery.
Methods: Using the National Cancer Data Base (1995-2004), 9559 patients were identified with potentially resectable tumors (pretreatment clinical Stage I: T1N0M0 and T2N0M0). Multivariate models were employed to identify factors predicting failure to undergo surgery and assess the impact of pancreatectomy on survival.
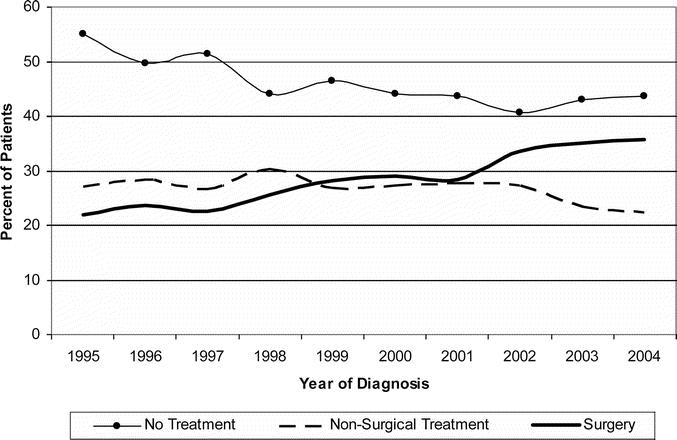
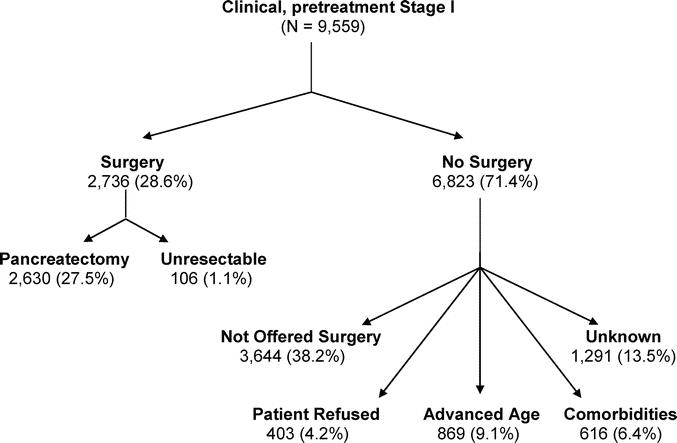
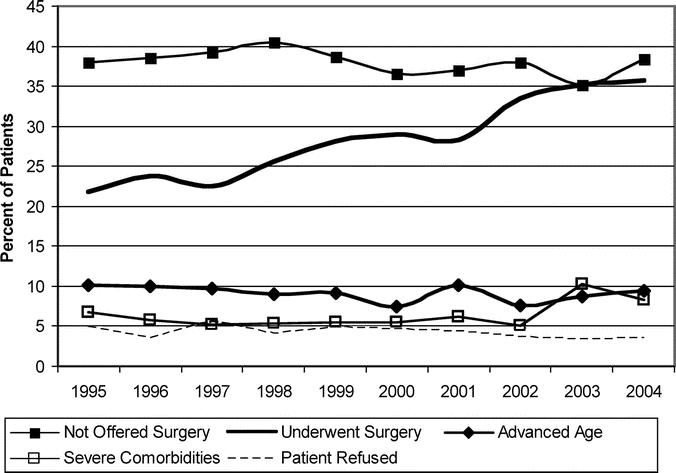
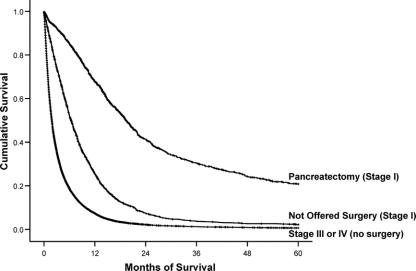
Results: Of clinical Stage I patients 71.4% (6823/9559) did not undergo surgery; 6.4% (616/9559) were excluded due to comorbidities; 4.2% (403/9559) refused surgery; 9.1% (869/9559) were excluded due to age; and 38.2% (3,644/9559) with potentially resectable cancers were classified as "not offered surgery." Of the 28.6% (2736/9559) of patients who underwent surgery, 96.0% (2630/2736) underwent pancreatectomy, and 4.0% (458/2736) had unresectable tumors. Patients were less likely to undergo surgery if they were older than 65 years, were black, were on Medicare or Medicaid, had pancreatic head lesions, earned lower annual incomes, or had less education (P < 0.0001). Patients were less likely to receive surgery at low-volume and community centers. Patients underwent surgery more frequently at National Cancer Institute/National Comprehensive Cancer Network-designated cancer centers (P < 0.0001). Patients who were not offered surgery had significantly better survival than those with Stage III or IV disease but worse survival than patients who underwent pancreatectomy for Stage I disease (P < 0.0001).
Conclusions: This is the first study to characterize the striking underuse of pancreatectomy in the United States. Of early stage pancreatic cancer patients without any identifiable contraindications, 38.2% failed to undergo surgery.
Figures
Comment in
-
Underutilization of surgical resection in patients with localized pancreatic cancer.Ann Surg. 2007 Aug;246(2):181-2. doi: 10.1097/SLA.0b013e31811eaa2c. Ann Surg. 2007. PMID: 17667494 Free PMC article. No abstract available.
-
Early pancreatic cancer: are we doing enough?Natl Med J India. 2007 Sep-Oct;20(5):243-4. Natl Med J India. 2007. PMID: 18254522 No abstract available.
References
-
- American Cancer Society: Cancer Facts and Figures. Available at http://www.cancer.org/docroot/stt/stt_0.asp. Accessed December 15, 2006.
-
- Brennan MF. Adjuvant therapy following resection for pancreatic adenocarcinoma. Surg Oncol Clin N Am. 2004;13:555–566, vii. - PubMed
-
- Stojadinovic A, Hoos A, Brennan MF, Conlon KC. Randomized clinical trials in pancreatic cancer. Surg Oncol Clin N Am. 2002;11:207–229, x. - PubMed
-
- Fernandez-del Castillo C, Rattner DW, Warshaw AL. Standards for pancreatic resection in the 1990s. Arch Surg. 1995;130:295–299, discussion 299–300. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
