

Postpancreatectomy hemorrhage: diagnosis and treatment: an analysis in 1669 consecutive pancreatic resections
- PMID: 17667506
- PMCID: PMC1933568
- DOI: 10.1097/01.sla.0000262953.77735.db
Postpancreatectomy hemorrhage: diagnosis and treatment: an analysis in 1669 consecutive pancreatic resections
Abstract
Background: To analyze clinical courses and outcome of postpancreatectomy hemorrhage (PPH) after major pancreatic surgery.
Summary background data: Although PPH is the most life-threatening complication following pancreatic surgery, standardized rules for its management do not exist.
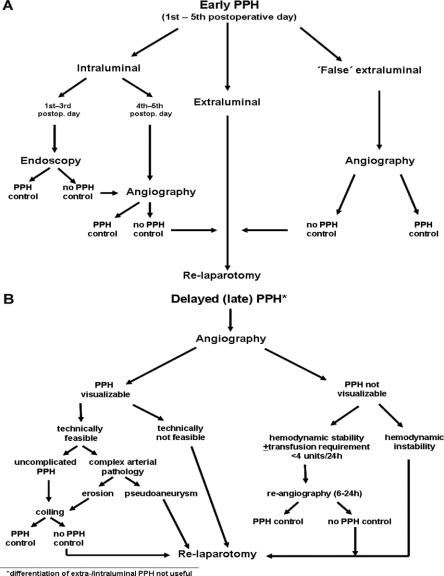
Methods: Between 1992 and 2006, 1524 patients operated on for pancreatic diseases were included in a prospective database. A risk stratification of PPH according to the following parameters was performed: severity of PPH classified as mild (drop of hemoglobin concentration <3 g/dL) or severe (>3 g/dL), time of PPH occurrence (early, first to fifth postoperative day; late, after sixth day), coincident pancreatic fistula, intraluminal or extraluminal bleeding manifestation, and presence of "complex" vascular pathologies (erosions, pseudoaneurysms). Success rates of interventional endoscopy and angiography in preventing relaparotomy were analyzed as well as PPH-related overall outcome.
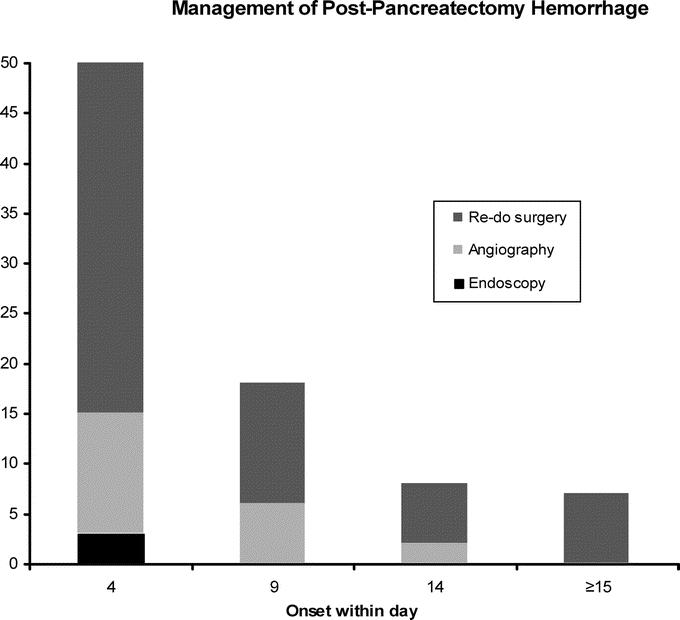
Results: Prevalence of PPH was 5.7% (n = 87) distributed almost equally among patients suffering from malignancies, borderline tumors, and focal pancreatitis (n = 47) and from chronic pancreatitis (n = 40). PPH-related overall mortality of 16% (n = 14) was closely associated with 1) the occurrence of pancreatic fistula (13 of 14); 2) vascular pathologies, ie, erosions and pseudoaneurysms (12 of 14); 3) delayed PPH occurrence (14 of 14); and 4) underlying disease with lethal PPH found only in patients with soft texture of the pancreatic remnant, while no patient with chronic pancreatitis died. Conversely, primary severity of PPH (mild vs. severe) and the kind of index operation (Whipple resection, pylorus-preserving partial pancreaticoduodenectomy, organ-preserving procedures) had no influence on outcome of PPH. Endoscopy was successful in 3 from 15 patients (20%), who had intraluminal PPH within the first or second postoperative day. "True," early extraluminal PPH had uniformly to be treated by relaparotomy. Seventeen patients had "false," early extraluminal PPH due to primarily intraluminal bleeding site from the pancreaticoenteric anastomosis with secondary disruption of the anastomosis. From 43 patients subjected to angiography, 25 underwent interventional coiling with a success rate of 80% (n = 20). Overall, relaparotomy was performed in 60 patients among whom 33 underwent surgery as first-line treatment, while 27 were relaparotomied as rescue treatment after failure of interventional endoscopy or radiology.
Conclusion: Prognosis of PPH depends mainly on the presence of preceding pancreatic fistula. Decision making as to the indication for nonsurgical interventions should consider time of onset, presence of pancreatic fistula, vascular pathologies, and the underlying disease.
Figures
References
-
- Izbicki JR, Bloechle C, Knoefel WT, et al. Surgical treatment of chronic pancreatitis and quality of life after operation. Surg Clin North Am. 1999;79:913–944. - PubMed
-
- Buchler MW, Wagner M, Schmied BM, et al. Changes in morbidity after pancreatic resection: toward the end of completion pancreatectomy. Arch Surg. 2003;138:1310–1314; discussion 1315. - PubMed
-
- van Berge Henegouwen MI, Allema JH, van Gulik TM, et al. Delayed massive haemorrhage after pancreatic and biliary surgery. Br J Surg. 1995;82:1527–1531. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
