

Predictors and outcome of gastrointestinal complications in patients undergoing cardiac surgery
- PMID: 17667513
- PMCID: PMC1933566
- DOI: 10.1097/SLA.0b013e3180603010
Predictors and outcome of gastrointestinal complications in patients undergoing cardiac surgery
Abstract
Objective: To determine the incidence and independent predictors of gastrointestinal complications (GICs) following cardiac surgery.
Summary background data: Gastrointestinal ischemia and hemorrhage represent a rare but devastating complication following heart surgery. The profile of patients referred for cardiac surgery has changed during the last decade, questioning the validity of previously reported incidence and risk factors.
Methods: We retrospectively analyzed prospectively collected data from 4819 patients undergoing cardiac surgery between 1998 and 2004. Patients with GICs were compared with the entire patient population. Study endpoints were mortality, postoperative morbidities, and long-term survival.
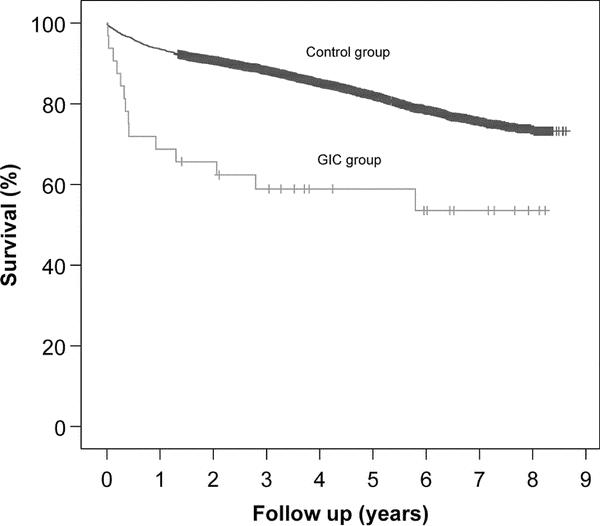
Results: GICs occurred in 51 (1.1%) patients. Etiologies were intestinal ischemia (n = 30; 59%) and hemorrhage (n = 21; 41%). The incidence decreased during the study period (1998-2001: 1.3%, 2002-2004: 0.7%; P = 0.04). The incidence per type of procedure was as follows: coronary artery bypass grafting (CABG)/valve (2.4%), aortic surgery (1.7%), valve surgery (1.0%), and CABG (0.5%; P = 0.001). Multivariate analysis revealed age (odds ratio [OR] = 2.1), myocardial infarction (OR = 2.5), CHF (OR = 2.4), hemodynamic instability (OR = 2.8), cardiopulmonary bypass time >120 minutes (OR = 6.2), peripheral vascular disease (OR = 2.2), renal (OR = 3.2), and hepatic failure (OR = 10.8) as independent predictors of GICs. The overall hospital mortality among patients with GICs was 33%. Long-term survival was significantly decreased in patients with GICs compared with the control group.
Conclusions: Gastrointestinal complications following cardiac surgery remain rare with an incidence <1% in a contemporary series. The key to a lower incidence of GICs lies in systematic application of preventive measures and new advances in intraoperative management. Identification of independent risk factors would facilitate the determination of patients who would benefit from additional perioperative monitoring. Future resources should therefore be redirected to mitigate GICs in high-risk patients.
Figures
References
-
- Christenson JT, Schmuziger M, Maurice J, et al. Postoperative visceral hypotension the common cause for gastrointestinal complications after cardiac surgery. Thorac Cardiovasc Surg. 1994;42:152–157. - PubMed
-
- Andersson B, Nilsson J, Brandt J, et al. Gastrointestinal complications after cardiac surgery. Br J Surg. 2005;92:326–333. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
