

Liver manipulation causes hepatocyte injury and precedes systemic inflammation in patients undergoing liver resection
- PMID: 17668263
- PMCID: PMC2039834
- DOI: 10.1007/s00268-007-9182-4
Liver manipulation causes hepatocyte injury and precedes systemic inflammation in patients undergoing liver resection
Abstract
Background: Liver failure following liver surgery is caused by an insufficient functioning remnant cell mass. This can be due to insufficient liver volume and can be aggravated by additional cell death during or after surgery. The aim of this study was to elucidate the causes of hepatocellular injury in patients undergoing liver resection.
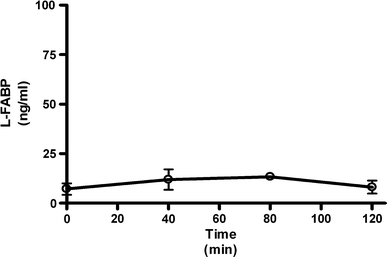
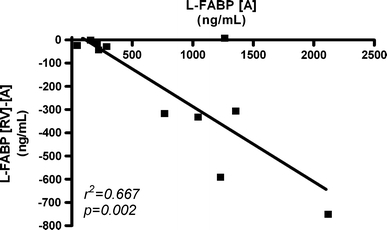
Methods: Markers of hepatocyte injury (AST, GSTalpha, and L-FABP) and inflammation (IL-6) were measured in plasma of patients undergoing liver resection with and without intermittent inflow occlusion. To study the separate involvement of the intestines and the liver in systemic L-FABP release, arteriovenous concentration differences for L-FABP were measured.
Results: During liver manipulation, liver injury markers increased significantly. Arterial plasma levels and transhepatic and transintestinal concentration gradients of L-FABP indicated that this increase was exclusively due to hepatic and not due to intestinal release. Intermittent hepatic inflow occlusion, anesthesia, and liver transection did not further enhance arterial L-FABP and GSTalpha levels. Hepatocyte injury was followed by an inflammatory response.
Conclusions: This study shows that liver manipulation is a leading cause of hepatocyte injury during liver surgery. A potential causal relation between liver manipulation and systemic inflammation remains to be established; but since the inflammatory response is apparently initiated early during major abdominal surgery, interventions aimed at reducing postoperative inflammation and related complications should be started early during surgery or beforehand.
Figures



References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/00000658-200102000-00011', 'is_inner': False, 'url': 'https://doi.org/10.1097/00000658-200102000-00011'}, {'type': 'PMC', 'value': 'PMC1421204', 'is_inner': False, 'url': 'https://pmc.ncbi.nlm.nih.gov/articles/PMC1421204/'}, {'type': 'PubMed', 'value': '11176128', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11176128/'}]}
- Wigmore SJ, Redhead DN, Yan XJ, et al. (2001) Virtual hepatic resection using three-dimensional reconstruction of helical computed tomography angioportograms. Ann Surg 233:221–226 - PMC - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/01.TP.0000144182.27897.1E', 'is_inner': False, 'url': 'https://doi.org/10.1097/01.tp.0000144182.27897.1e'}, {'type': 'PubMed', 'value': '15599312', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15599312/'}]}
- Patel A, van de Poll MC, Greve JW, et al. (2004) Early stress protein gene expression in a human model of ischemic preconditioning. Transplantation 78:1479–1487 - PubMed
-
- None
- Boschetto A, Dondero F, Tonini V, et al. (2005) Intra-operative liver injury is not only related to vascular clamping [abstract]. HPB 7:P25
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1093/bja/48.2.119', 'is_inner': False, 'url': 'https://doi.org/10.1093/bja/48.2.119'}, {'type': 'PubMed', 'value': '3192', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/3192/'}]}
- Clarke RS, Doggart JR, Lavery T (1976) Changes in liver function after different types of surgery. Br J Anaesth 48:119–128 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1002/bjs.5224', 'is_inner': False, 'url': 'https://doi.org/10.1002/bjs.5224'}, {'type': 'PubMed', 'value': '16392101', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/16392101/'}]}
- Hiki N, Shimizu N, Yamaguchi H, et al. (2006) Manipulation of the small intestine as a cause of the increased inflammatory response after open compared with laparoscopic surgery. Br J Surg 93:195–204 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
