

Autotransfusion management during and after cardiopulmonary bypass alters fibrin degradation and transfusion requirements
- PMID: 17672185
- PMCID: PMC4680668
Autotransfusion management during and after cardiopulmonary bypass alters fibrin degradation and transfusion requirements
Abstract
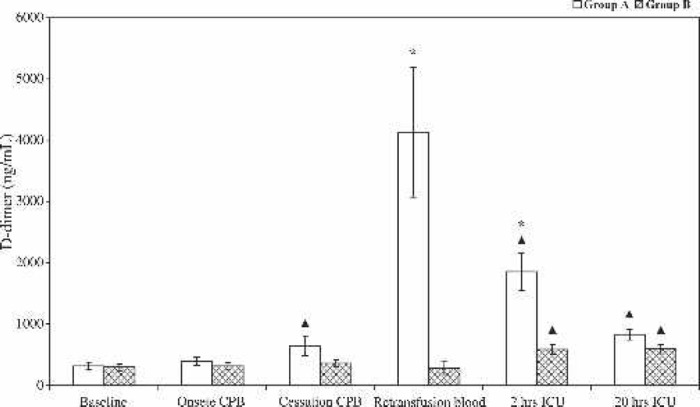
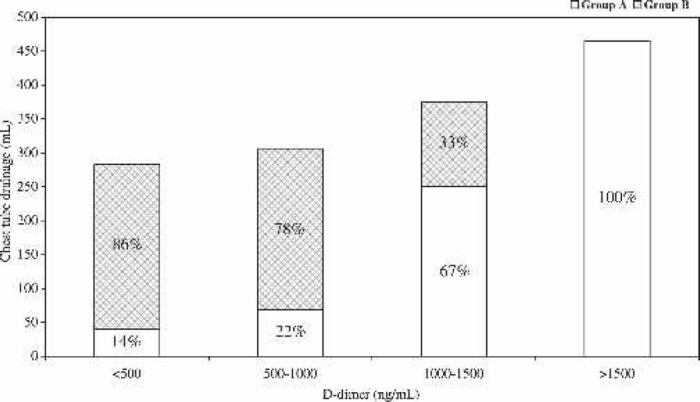
The coagulation-fibrinolytic profile during cardiopulmonary bypass (CPB) has been widely documented. However, less information is available on the possible persistence of these alterations when autotransfusion is used in management of perioperative blood loss. This study was designed to explore the influence of autotransfusion management on intravascular fibrin degradation and postoperative transfusions. Thirty patients, undergoing elective primary isolated coronary bypass grafting, were randomly allocated either to a control group (group A; n=15) or an intervention group (group B; n=15) in which mediastinal and residual CPB blood was collected and processed by a continuous autotransfusion system before re-infusion. Intravascular fibrin degradation as indicated by D-dimer generation was measured at five specific intervals and corrected for hemodilution. In addition, chest tube drainage and need for homologous blood were monitored. D-dimer generation increased significantly during CPB in group A, from 312 to 633 vs. 291 to 356 ng/mL in group B (p = .001). The unprocessed residual blood (group A) revealed an unequivocal D-dimer elevation, 4131 +/- 1063 vs. 279 +/- 103 ng/mL for the processed residual in group B (p < .001). Consequently, in the first post-CPB period, the intravascular fibrin degradation was significantly elevated in group A compared with group B (p = .001). Twenty hours postoperatively, no significant difference in D-dimer levels was detected between both groups. However, a significant intra-group D-dimer elevation pre- vs. postoperative was noticed from 312 to 828 ng/mL in group A and from 291 to 588 ng/mL in group B (p < .01 for both). Postoperative chest tube drainage was higher in the patients from group A, which also had the highest postoperative D-dimer levels. Patients in group A perceived a higher need for transfusions of red cells suspensions postoperatively. These data clearly indicate that autotransfusion management during and after CPB suppresses early postoperative fibrin degradation.
Keywords: cardiopulmonary bypass, cardiotomy suction, coronary surgery, autotransfusion, fibrin degradation.
Conflict of interest statement
The senior author has stated that authors have reported no material, financial or other relationship with any healthcare-related business or other entity whose products or services are discussed in this paper.
Figures
Similar articles
-
Closed cardiopulmonary bypass circuits suppress thrombin generation during coronary artery bypass grafting.Interact Cardiovasc Thorac Surg. 2010 Apr;10(4):555-60. doi: 10.1510/icvts.2009.214437. Epub 2010 Jan 8. Interact Cardiovasc Thorac Surg. 2010. PMID: 20061337 Clinical Trial.
-
Effects of cell saver autologous blood transfusion on blood loss and homologous blood transfusion requirements in patients undergoing cardiac surgery on- versus off-cardiopulmonary bypass: a randomised trial.Eur J Cardiothorac Surg. 2006 Aug;30(2):271-7. doi: 10.1016/j.ejcts.2006.04.042. Epub 2006 Jul 7. Eur J Cardiothorac Surg. 2006. PMID: 16829083 Clinical Trial.
-
Does heparin pretreatment affect the haemostatic system during and after cardiopulmonary bypass?Perfusion. 2001 Jan;16(1):3-12. doi: 10.1177/026765910101600102. Perfusion. 2001. PMID: 11192305 Clinical Trial.
-
Intraoperative and postoperative blood salvage.AACN Clin Issues. 1996 May;7(2):238-48. doi: 10.1097/00044067-199605000-00007. AACN Clin Issues. 1996. PMID: 8718386 Review.
-
Autotransfusion and blood conservation in urologic oncology.Semin Surg Oncol. 1989;5(4):286-92. doi: 10.1002/ssu.2980050412. Semin Surg Oncol. 1989. PMID: 2672235 Review.
Cited by
-
Cell salvage for minimising perioperative allogeneic blood transfusion in adults undergoing elective surgery.Cochrane Database Syst Rev. 2023 Sep 8;9(9):CD001888. doi: 10.1002/14651858.CD001888.pub5. Cochrane Database Syst Rev. 2023. PMID: 37681564 Free PMC article.
-
Blood transfusion practices in cardiac anaesthesia.Indian J Anaesth. 2014 Sep;58(5):616-21. doi: 10.4103/0019-5049.144669. Indian J Anaesth. 2014. PMID: 25535425 Free PMC article. Review.
-
The Hemobag: the modern ultrafiltration system for patients undergoing cardiopulmonary by pass.J Cardiothorac Surg. 2012 Jun 14;7:55. doi: 10.1186/1749-8090-7-55. J Cardiothorac Surg. 2012. PMID: 22697396 Free PMC article.
-
Cell salvage for minimising perioperative allogeneic blood transfusion.Cochrane Database Syst Rev. 2010 Apr 14;2010(4):CD001888. doi: 10.1002/14651858.CD001888.pub4. Cochrane Database Syst Rev. 2010. Update in: Cochrane Database Syst Rev. 2023 Sep 8;9:CD001888. doi: 10.1002/14651858.CD001888.pub5. PMID: 20393932 Free PMC article. Updated.
-
The effect of salvaged blood on coagulation function as measured by thromboelastography.Transfusion. 2013 Jun;53(6):1235-9. doi: 10.1111/j.1537-2995.2012.03884.x. Epub 2012 Aug 31. Transfusion. 2013. PMID: 22934712 Free PMC article. Clinical Trial.
References
-
- Paparella D, Brister SJ, Buchanan MR.. Coagulation disorders of cardiopulmonary bypass: A review. Intensive Care Med. 2004;30:1873–81. - PubMed
-
- Gunaydin S.. Clinical significance of coated extracorporeal circuits: A review of novel technologies. Perfusion. 2004;19:S33–41. - PubMed
-
- Wan S, LeClerc J-L, Vincent J-L.. Inflammatory response to cardiopulmonary bypass: Mechanisms involved and possible therapeutic strategies. Chest. 1997;112:676–92. - PubMed
-
- Aldea GS, Soltow LO, Chandler WL, et al. . Limitation of thrombin generation, platelet activation, and inflammation by elimination of cardiotomy suction in patients undergoing coronary artery bypass grafting treated with heparin-bonded circuits. J Thorac Cardiovasc Surg. 2002;123:742–55. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources