

Orthotopic liver transplantation in ninety-three patients
- PMID: 176741
- PMCID: PMC2605292
Orthotopic liver transplantation in ninety-three patients
Abstract
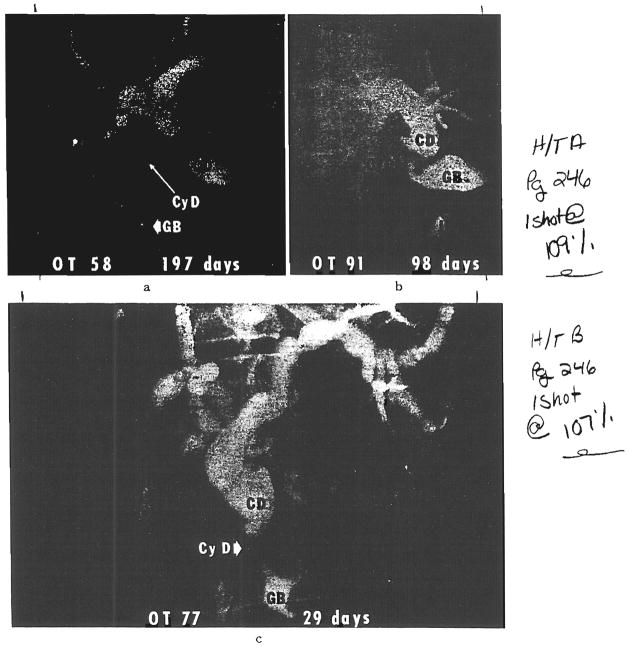
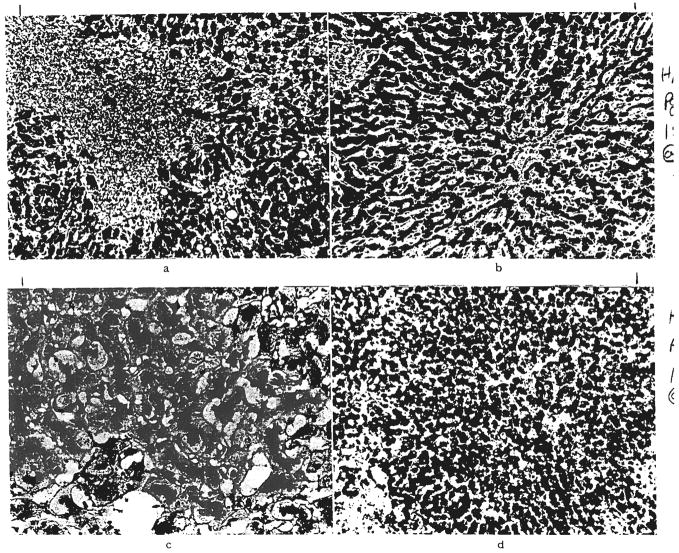
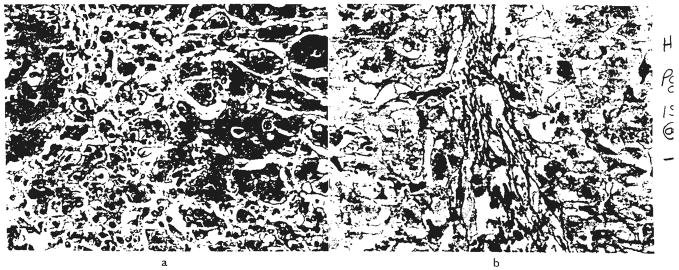
During the 11 1/2 year period ending 13 months ago, 93 consecutive patients were treated with orthotopic liver transplantation. Fifty-six of the recipients were 18 years old or younger, and the other 37 were adults. The most common indications for operation were biliary atresia, primary hepatic malignant tumor, chronic aggressive hepatitis and alcoholic cirrhosis. There has been a gradual improvement in results throughout the period of study, although to a satisfactory level. Twenty-seven of the 93 patients survived for at least one year after liver replacement with a maximum of six years, and 16 are still alive after 13 to 71 months. The 11 late deaths after one to six years were caused by chronic rejection, biliary obstruction, recurrence of hepatoma, systemic infection or hepatitis of the homograft. Rejection of the liver as judged by classical histopathologic criteria played a surprisingly small role in the heavy over-all mortality, accounting for less than 10 per cent of the deaths. Technical or mechanical problems, especially those of biliary duct reconstruction, were a far greater cause of failure, as were systemic infections. Six of the 37 adult recipients had lethal cerebrovascular accidents during, or just after, operation. When abnormalities of liver function developed in the postoperative period, the nearly automatic diagnosis of homograft rejection, in retrospect, proved to have been wrong in most instances. Further development of liver transplantation depends upon two kinds of progress. There must be reduction of operative and early postoperative accidents and complications by more discriminating patient selection, purely technical improvement and better standardization of biliary duct reconstruction. The second area will be in sharpening the criteria for the differnetial diagnosis of postoperative hepatic malfunction, including the liberal use of transhepatic cholangiography and needle biopsy. Only then can better decisions be made about changes in medication or about the need for secondary corrective surgical procedures.
Figures

References
-
- Alican F, Hardy J. Replantation of the liver in dogs. J Surg Res. 1967;7:368.
-
- Battersby C, Egerton WS, Balderson G, et al. Another look at rejection in pig liver homografts. Surgery. 1974;76:617. - PubMed
-
- Berne TV, Chatterjee SN, Craig JR, et al. Hepatic dysfunction in recipients of renal allografts. Surg Gynecol Obstet. 1975;141:171. - PubMed
-
- Birtch AG, Moore FD. Experience in liver transplantation. Transplant Rev. 1969;2:90. - PubMed
-
- Blumberg BS, Gerstley BJS, Hungerford DA, et al. A serum antigen (Australia antigen) in Down’s syndrome, leukemia, and hepatitis. Ann Intern Med. 1967;66:924. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources