

Detecting early pancreatic cancer: problems and prospects
- PMID: 17674956
- PMCID: PMC2680914
- DOI: 10.1053/j.seminoncol.2007.05.005
Detecting early pancreatic cancer: problems and prospects
Abstract
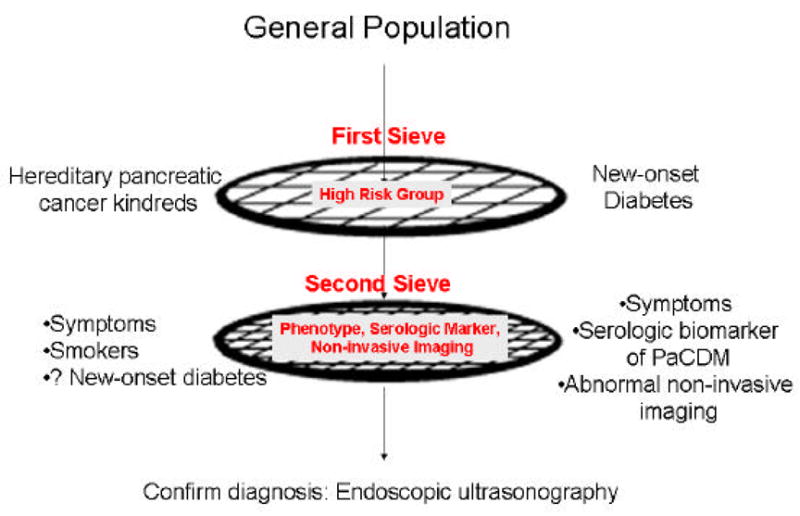
Pancreatic cancer has a poor prognosis. Improving survival will require diagnosis of early pancreatic cancer, which can be defined based on resectability, size, or curability. Pancreatic cancer progresses from noninvasive precursor lesions to invasive cancer over a variable time period. Retrospective review of computed tomography (CT) scans performed prior to diagnosis suggests that pancreatic cancer resectability may be significantly improved if detected as few as 6 months before clinical diagnosis. Since pancreatic cancer is relatively uncommon, to allow cost-effective screening the populations will have to be enriched for the disease using two "sieves." The first sieve would identify a population of subjects at higher than average risk of pancreatic cancer and the second sieve could be a characteristic phenotype among the members of the high-risk group, an abnormality seen on noninvasive imaging or a serologic marker of early pancreatic cancer. So far two high-risk groups have been targets of screening for pancreatic cancer: hereditary pancreatic cancer kindreds and new-onset diabetes. There is no serologic marker of early pancreatic cancer. Confirmation of diagnosis usually requires invasive procedures such as endoscopic ultrasonography (EUS). Although much work still needs to be done, the developments in the field provide us with hope that screening for early pancreatic cancer could become a reality in the not-so-distant future.
Figures




References
-
- Jemal AMT, Ward E, Samuels A, Tiwari RC, Ghafoor A, Feuer EJ, Thun MJ. Cancer Statistics, 2005. CA Cancer J Clin. 2005;55:10–30. - PubMed
-
- Maire F, Sauvanet A, Trivin F, et al. Staging of pancreatic head adenocarcinoma with spiral CT and endoscopic ultrasonography: an indirect evaluation of the usefulness of laparoscopy. Pancreatology. 2004;4:436–40. - PubMed
-
- Karmazanovsky G, Fedorov V, Kubyshkin V, et al. Pancreatic head cancer: accuracy of CT in determination of resectability. Abdom Imaging. 2005;30:488–500. - PubMed
-
- Roche CJ, Hughes ML, Garvey CJ, et al. CT and pathologic assessment of prospective nodal staging in patients with ductal adenocarcinoma of the head of the pancreas. AJR Am J Roentgenol. 2003;180:475–80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
