

Radical cystectomy: defining the threshold for a surgeon to achieve optimum outcomes
- PMID: 17675551
- PMCID: PMC2600107
- DOI: 10.1136/pgmj.2007.058214
Radical cystectomy: defining the threshold for a surgeon to achieve optimum outcomes
Abstract
Background: The reorganisation of cancer services in England will result in the creation of specialist high volume cancer surgery centres. Studies have suggested a relationship between increasing surgical volume and improved outcomes in urological pelvic cancer surgery, although to date, they have pre-defined the definition of "high" and "low" volume surgeons.
Aim: To derive the minimum caseload a surgeon requires to achieve optimum outcomes and to examine the effect of the operating centre size upon individual surgeon's outcomes.
Methods: All cystectomies performed for bladder cancer in England over 5 years were analysed from Hospital Episode Statistics (HES) data. Statistical analysis was undertaken to describe the relationship between each surgeon's annual case volume and two
Outcome measures: in-hospital mortality rate, and hospital stay. The surgeon's outcomes were then analysed with respect to the overall level of activity in their operating centre.
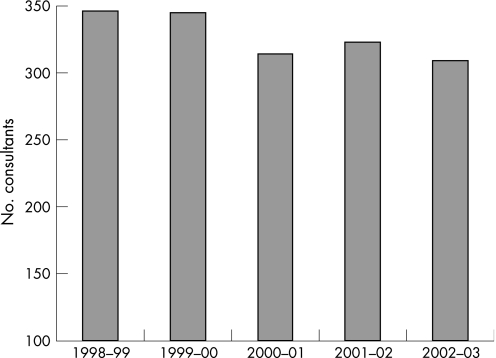
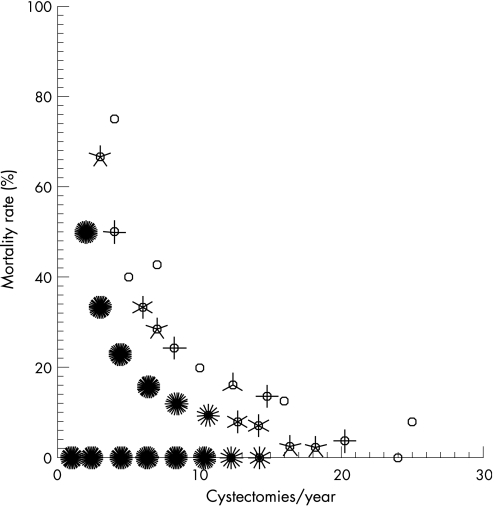
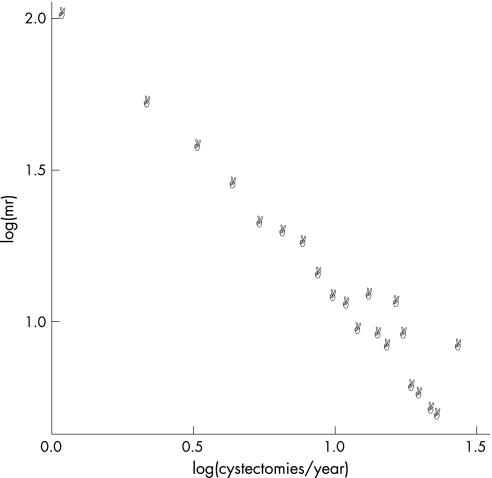
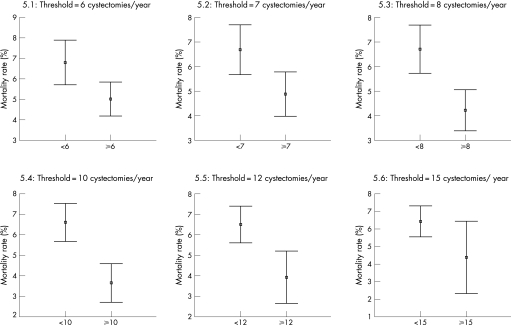
Results: A total of 6308 cystectomies were performed; the mean number of surgeons performing them annually was 327 with an overall mortality rate of 5.53%. A significant inverse correlation (-0.968, p<0.01) was found between case volume and mortality rate. Applying 95% confidence interval estimation, the minimum caseload required to achieve the lowest mortality rate was eight procedures per year. Increasing caseload beyond eight operations per year did not produce a significant reduction in mortality rate.
Conclusion: Analysis of HES data confirms an inverse relationship between surgeon's caseload and mortality for radical cystectomy. A caseload of eight operations per year is associated with the lowest mortality rate.
Conflict of interest statement
Competing interests: None declared
Similar articles
-
Defining the minimum hospital case-load to achieve optimum outcomes in radical cystectomy.BJU Int. 2005 Oct;96(6):806-10. doi: 10.1111/j.1464-410X.2005.05717.x. BJU Int. 2005. PMID: 16153206
-
Provision of radical pelvic urological surgery in England, and compliance with improving outcomes guidance.BJU Int. 2009 Nov;104(10):1446-51. doi: 10.1111/j.1464-410X.2009.08614.x. Epub 2009 Jun 22. BJU Int. 2009. PMID: 19549126
-
Association of procedure volume with radical cystectomy outcomes in a nationwide database.J Urol. 2007 Oct;178(4 Pt 1):1418-21; discussion 1421-2. doi: 10.1016/j.juro.2007.05.156. Epub 2007 Aug 16. J Urol. 2007. PMID: 17706712
-
Influence of caseload and surgical speciality on outcome following surgery for colorectal cancer: a review of evidence. Part 2: long-term outcome.Colorectal Dis. 2007 Jan;9(1):38-46. doi: 10.1111/j.1463-1318.2006.01095.x. Colorectal Dis. 2007. PMID: 17181844 Review.
-
Influence of caseload and surgical speciality on outcome following surgery for colorectal cancer: a review of evidence. Part 1: short-term outcome.Colorectal Dis. 2007 Jan;9(1):28-37. doi: 10.1111/j.1463-1318.2006.01100.x. Colorectal Dis. 2007. PMID: 17181843 Review.
Cited by
-
Diagnosis and management of intradiverticular bladder tumours.Nat Rev Urol. 2014 Jul;11(7):383-90. doi: 10.1038/nrurol.2014.131. Epub 2014 Jun 17. Nat Rev Urol. 2014. PMID: 24934450 Review.
-
Urinary diversion practice patterns among certifying American urologists.J Urol. 2013 Mar;189(3):1042-7. doi: 10.1016/j.juro.2012.08.240. Epub 2012 Sep 23. J Urol. 2013. PMID: 23009870 Free PMC article.
-
Surgical margin status among men with organ-confined (pT2) prostate cancer: a population-based study.Can Urol Assoc J. 2011 Jun;5(3):161-6. doi: 10.5489/cuaj.10085. Can Urol Assoc J. 2011. PMID: 21672475 Free PMC article.
-
Predictors of referral for neoadjuvant chemotherapy prior to radical cystectomy for muscle-invasive bladder cancer and changes in practice over time.Can Urol Assoc J. 2015 Jul-Aug;9(7-8):236-41. doi: 10.5489/cuaj.2722. Can Urol Assoc J. 2015. PMID: 26316905 Free PMC article.
-
Assessing the relative influence of hospital and surgeon volume on short-term mortality after radical cystectomy.BJU Int. 2017 Aug;120(2):239-245. doi: 10.1111/bju.13804. Epub 2017 Mar 10. BJU Int. 2017. PMID: 28192632 Free PMC article.
References
-
- Singh R, O'Brien T S. The relationship between volume and outcome in urological surgery. BJU Int 200493931–935. - PubMed
-
- National Institute for Health and Clinical Excellence Improving outcomes in urological cancer. London: NICE, 2002, http://www.nice.org.uk
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
