

Growth hormone axis in chronic kidney disease
- PMID: 17676425
- PMCID: PMC2100434
- DOI: 10.1007/s00467-007-0527-x
Growth hormone axis in chronic kidney disease
Abstract
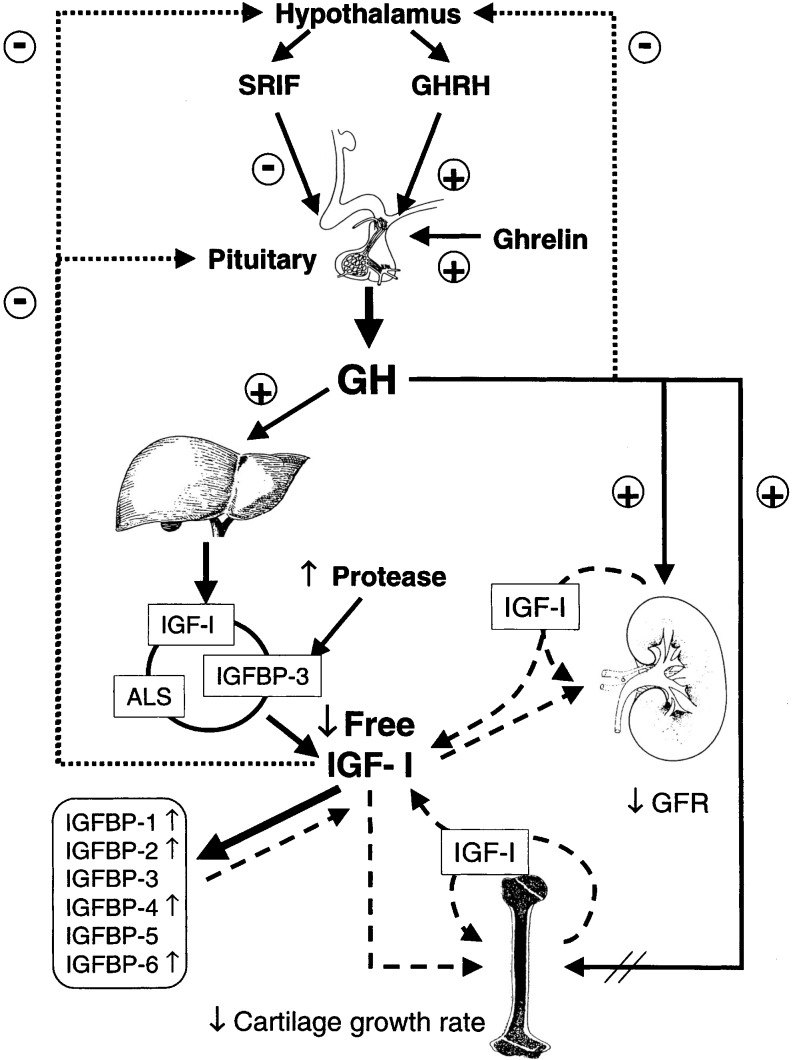
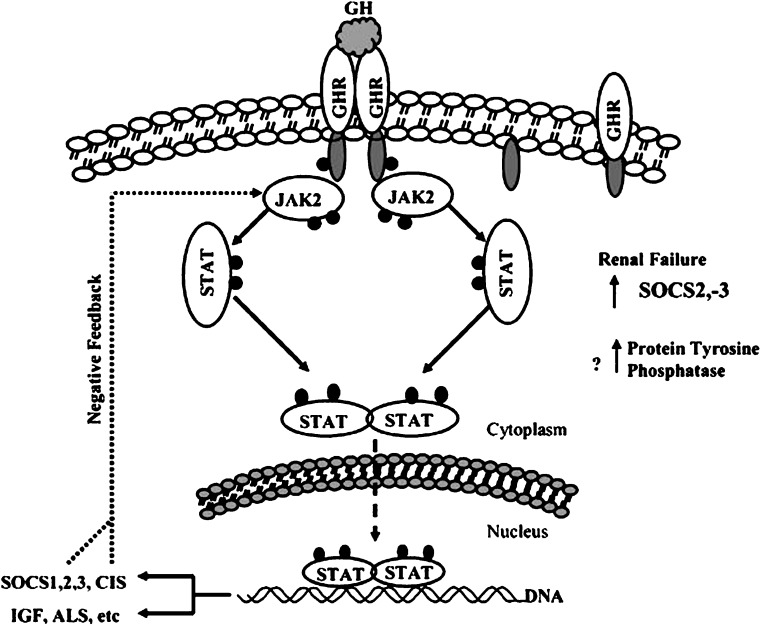
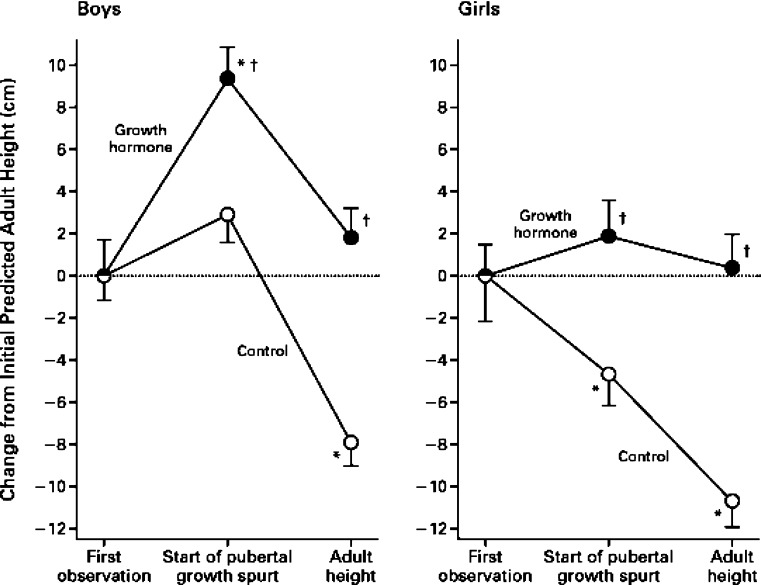
Chronic kidney disease (CKD) in children is associated with dramatic changes in the growth hormone (GH) and insulin-like growth factor (IGF-1) axis, resulting in growth retardation. Moderate-to-severe growth retardation in CKD is associated with increased morbidity and mortality. Renal failure is a state of GH resistance and not GH deficiency. Some mechanisms of GH resistance are: reduced density of GH receptors in target organs, impaired GH-activated post-receptor Janus kinase/signal transducer and activator of transcription (JAK/STAT) signaling, and reduced levels of free IGF-1 due to increased inhibitory IGF-binding proteins (IGFBPs). Treatment with recombinant human growth hormone (rhGH) has been proven to be safe and efficacious in children with CKD. Even though rhGH has been shown to improve catch-up growth and to allow the child to achieve normal adult height, the final adult height is still significantly below the genetic target. Growth retardation may persist after renal transplantation due to multiple factors, such as steroid use, decreased renal function and an abnormal GH-IGF1 axis. Those below age 6 years are the ones to benefit most from transplantation in demonstrating acceleration in linear growth. Newer treatment modalities targeting the GH resistance with recombinant human IGF-1 (rhIGF-1), recombinant human IGFBP3 (rhIGFBP3) and IGFBP displacers are under investigation and may prove to be more effective in treating growth failure in CKD.
Figures
References
-
- Haffner D, Schaefer F, Nissel R, Wuhl E, Tonshoff B, Mehls O. Effect of growth hormone treatment on the adult height of children with chronic renal failure. German Study Group for Growth Hormone Treatment in Chronic Renal Failure. N Engl J Med. 2000;343(13):923–9.0. - PubMed
-
- Seikaly MG, Salhab N, Gipson D, Yiu V, Stablein D. Stature in children with chronic kidney disease: analysis of NAPRTCS database. Pediatr Nephrol. 2006;21(6):793–799. - PubMed
-
- Mahan JD, Warady BA, the Consensus Committee Assessment and treatment of short stature in pediatric patients with chronic kidney disease: a consensus statement. Pediatr Nephrol. 2006;21(7):917–930. - PubMed
-
- North American Pediatric Renal Transplant Cooperative Study (2005) Annual report. Available at https://doi.org/spitfire.emmes.com/study/ped/resources/annlrept2005.pdf
-
- Furth SL, Hwang W, Yang C, Neu AM, Fivush BA, Powe NR. Growth failure, risk of hospitalization and death for children with end-stage renal disease. Pediatr Nephrol. 2002;17(6):450–455. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
