

Greater trochanteric pain syndrome: epidemiology and associated factors
- PMID: 17678660
- PMCID: PMC2907104
- DOI: 10.1016/j.apmr.2007.04.014
Greater trochanteric pain syndrome: epidemiology and associated factors
Abstract
Objectives: To describe the prevalence of greater trochanteric pain syndrome (GTPS); to determine whether GTPS is associated with iliotibial band (ITB) tenderness, knee osteoarthritis (OA), body mass index (BMI), or low back pain (LBP); and to assess whether GTPS is associated with reduced hip internal rotation, physical activity, and mobility.
Design: Cross-sectional, population-based study.
Setting: Multicenter observational study.
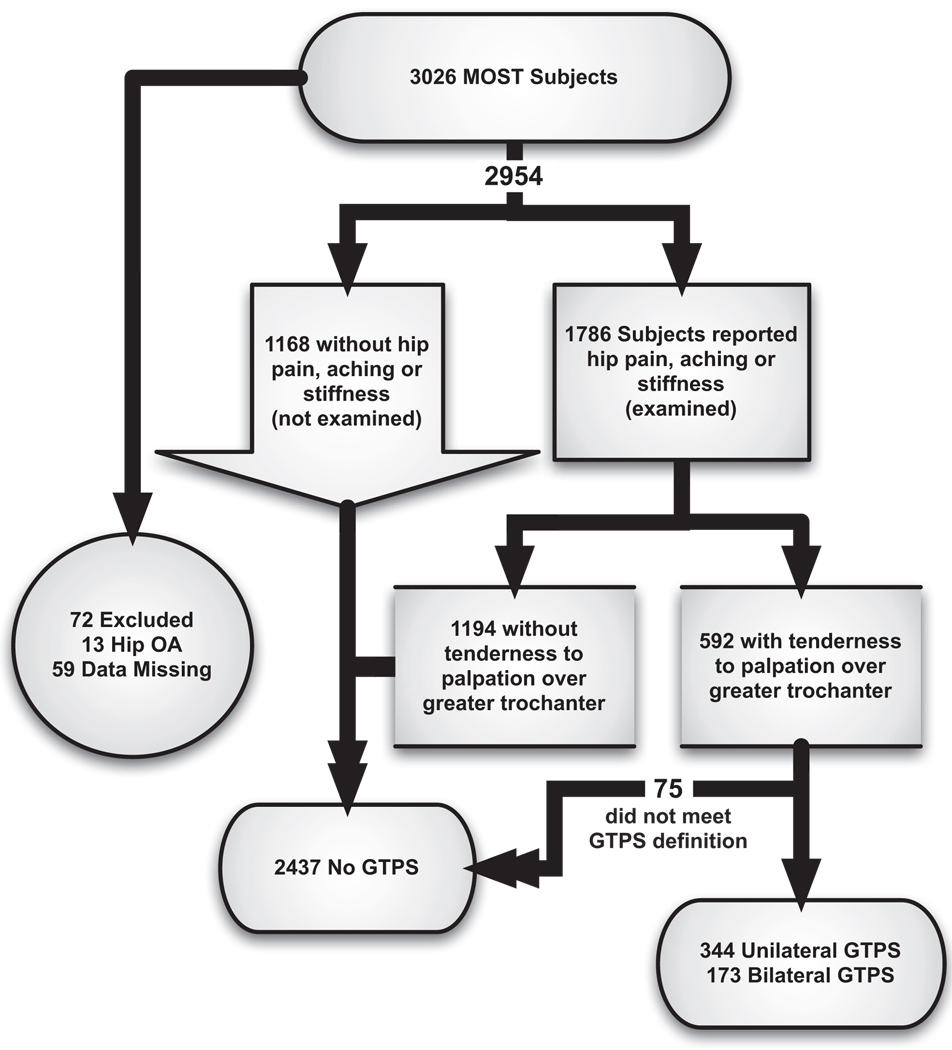
Participants: Community-dwelling adults (N=3026) ages 50 to 79 years.
Interventions: Not applicable.
Main outcome measures: Greater trochanteric tenderness to palpation in subjects with complaints of hip pain and no signs of hip OA or generalized myofascial tenderness.
Results: The prevalence of unilateral and bilateral GTPS was 15.0% and 8.5% in women and 6.6% and 1.9% men. Odds ratio (OR) for women was 3.37 (95% confidence interval [CI], 2.67-4.25), but age and race were not significantly associated with GTPS. In a multivariate model, adjusting for age, sex, ITB tenderness, ipsilateral and contralateral knee OA, BMI, and LBP, ITB tenderness (OR=1.72; 95% CI, 1.34-2.19), knee OA ipsilaterally (OR=3.47; 95% CI, 2.72-4.42) and contralaterally (OR=1.74; 95% CI, 1.32-2.28), and LBP (OR=2.79; 95% CI, 2.22-3.50) were positively related to GTPS. In this complete model, BMI was not associated with GTPS (OR=1.10; 95% CI, 0.80-1.52 when comparing >or=30 with <25kg/m(2)). Hip internal rotation range of motion did not differ based on GTPS status. After multivariate adjustment, GTPS did not alter physical activity score, but bilateal GTPS was significantly associated with a higher 20-meter walk time and chair stand time.
Conclusions: The higher prevalence of GTPS in women and in adults with ITB pain or knee OA indicates that altered lower-limb biomechanics may be related to GTPS. Slower functional performance in those with GTPS suggests that the study of targeted rehabilitation may be useful. A longitudinal study will be necessary to identify causal factors and outcomes of interventions.
References
-
- Shapira D, Nahir M, Shcharf Y. Trochanteric bursitis: a common clinical problem. Arch Phys Med Rehabil. 1986;67:815–817. - PubMed
-
- Shbeeb MI, Matteson EL. Trochanteric bursitis (greater trochanter pain syndrome) Mayo Clin Proc. 1996;71:565–569. - PubMed
-
- Lequesne M. From “periarthritis” to hip “rotator cuff” tears. Trochanteric tendinobursitis. Joint Bone Spine. 2006;73:344–348. - PubMed
-
- Bird PA, Oakley SP, Shnier R, Kirkham BW. Prospective evaluation of magnetic resonance imaging and physical examination findings in patients with greater trochanteric pain syndrome. Arthritis Rheum. 2001;44:2138–2145. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
