

Review
doi: 10.1016/j.nuclcard.2007.05.006.
Role of PET in the evaluation and understanding of coronary physiology
Affiliations
- PMID: 17679069
- PMCID: PMC1995749
- DOI: 10.1016/j.nuclcard.2007.05.006
Item in Clipboard
Review
Role of PET in the evaluation and understanding of coronary physiology
J Nucl Cardiol.
2007 Jul.
No abstract available
Figures

(A) Normal coronary angiogram of the left coronary tree in the RAO view of a healthy individual without coronary risk factors. (B) Corresponding angiogram during sympathetic stimulation with CPT. (C and D) Quantitative angiographic assessment of the proximal-mid LAD segment at rest (mean diameter: 2.0mm) (C) and during CPT (mean diameter:2.5mm) (D). (With kind permission from reference 49)
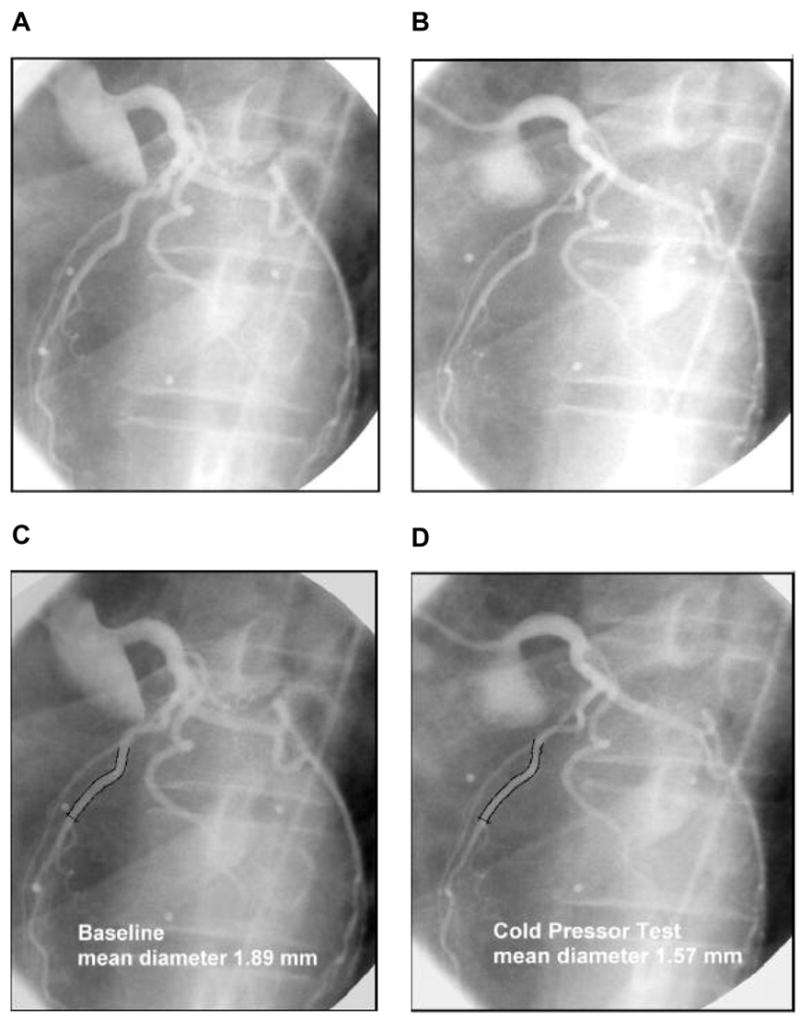
(A) Normal coronary angiogram of the left coronary artery tree in the LAO view in a chronic smkokers at rest. (B) Corresponding coronary angiogram during CPT. (C and D) Quantitative angiographic assessment of the proximal-mid LAD segment at rest (mean diameter: 1.89mm) (C) and during CPT (mean diameter:1.57mm) (D). (With kind permission from reference 49)

Association between the coronary flow response to CPT and actylcholine stimulation during coronary angiography in 12 normal control patients and in 19 patients with diffuse CAD. The CPT-induced changes in coronary vascular resistance inversely and significantly correlateds with the extent of endothelial dysfunction of the coronary arteriolar vessels as determined with acetylcholine stimulation. (With kind permission from reference 53)

Hyperaemic MBF increase to adenosine stimulation and its alteration to the intravenous infusion of the nitric oxide (NO) synthase inhibitor NG-nitro-L-arginine methyl ester (4mg L-NAME /body weight i.v.). In the presence of L-NAME the hyperaemic MBF response was attenuated by 21% that is likely to reflect the impairment of the flow-mediated and, thus, endothelium-derived and NO-mediated vasodilation by L-NAME. (Adapted from reference 67)
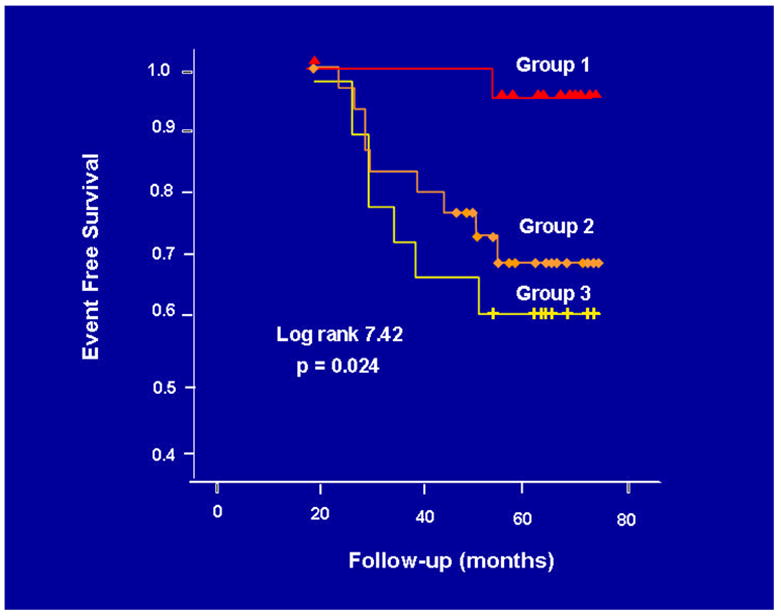
Prognostic value of PET-measured, endothelium-related MBF responses to sympathetic stimulation with CPT. The Kaplan-Meier analysis demonstrates an association between the incidence of cardiovascular events and the degree of the dimished MBF response to CPT (group 1: ?MBF ≥40%; group 2: ?MBF<40% and; group 3: ?MBF≤0%). (With kind permission from reference 9)

Effects of short-term and long-term antioxidant intervention on endothelium-related MBF responses to CPT. The graphic demonstrates contrasting MBF responses to challenges in vitamin C in hypercholesterolemic patients, smokers and hypertensive patients. (With kind permission from reference 15)

(A) Myocardial blood flow (MBF) at rest, during cold pressor testing (CPT), and during pharmacologic vasodilation with dipyridamole for the three study groups. The dipyridamole-stimulated MBF was lower in overweight than in controls, but not significantly. In obesity the hyperaemic MBFs during dipyridamole stimulation were lowest. (B) Change of endothelium-related MBF during CPT (?MBF) for the three study groups. As can be appreciated, there is a progressive decrease of the endothelium-related MBF response to CPT from control, to overweight and obesity. (With kind permission from reference 18).

(A) Myocardial blood flow (MBF) at rest, during cold pressor testing (CPT), and during pharmacologic vasodilation with dipyridamole for the three study groups. The dipyridamole-stimulated MBF was lower in overweight than in controls, but not significantly. In obesity the hyperaemic MBFs during dipyridamole stimulation were lowest. (B) Change of endothelium-related MBF during CPT (?MBF) for the three study groups. As can be appreciated, there is a progressive decrease of the endothelium-related MBF response to CPT from control, to overweight and obesity. (With kind permission from reference 18).

(A) Effects of glucose lowering-therapy with glyburide and metformin on endothelium-related ?MBF to CPT in type 2 diabetes mellitus patients. In type 2 diabetic patients with euglycemic control after 3 months of glucose lowering treatment with glucose plasma levels ≤126mg/dl (group of responders) the endothelium-mediated MBF response to CPT significantly increased comparable to controls, while in patients with glucose plasma levels >126mg/dl (group of non- responders) virtually no change in ?MBF to CPT was observed. (B) Association of the endothelium-related ?MBF to CPT and the change in fasting plasma glucose concentration as defined as difference in ?MBF and ?Glucose decrease between 3 months follow-up and baseline measurements. (With kind permission from reference 21)

(A) Effects of glucose lowering-therapy with glyburide and metformin on endothelium-related ?MBF to CPT in type 2 diabetes mellitus patients. In type 2 diabetic patients with euglycemic control after 3 months of glucose lowering treatment with glucose plasma levels ≤126mg/dl (group of responders) the endothelium-mediated MBF response to CPT significantly increased comparable to controls, while in patients with glucose plasma levels >126mg/dl (group of non- responders) virtually no change in ?MBF to CPT was observed. (B) Association of the endothelium-related ?MBF to CPT and the change in fasting plasma glucose concentration as defined as difference in ?MBF and ?Glucose decrease between 3 months follow-up and baseline measurements. (With kind permission from reference 21)
References
-
- Kuhle WG, Porenta G, Huang SC, Buxton D, Gambhir SS, Hansen H, et al. Quantification of regional myocardial blood flow using 13N-ammonia and reoriented dynamic positron emission tomographic imaging. Circulation. 1992;86(3):1004–1017. - PubMed
-
- Kaufmann PA, Camici PG. Myocardial blood flow measurement by PET: technical aspects and clinical applications. J Nucl Med. 2005;46(1):75–88. - PubMed
-
- Schelbert HR, Phelps ME, Huang SC, MacDonald NS, Hansen H, Selin C, et al. N-13 ammonia as an indicator of myocardial blood flow. Circulation. 1981;63(6):1259–1272. - PubMed
-
- Bergmann SR, Fox KA, Rand AL, McElvany KD, Welch MJ, Markham J, et al. Quantification of regional myocardial blood flow in vivo with H215O. Circulation. 1984;70(4):724–733. - PubMed
-
- Camici PG, Crea F. Coronary microvascular dysfunction. N Engl J Med. 2007;356(8):830–840. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
