

Clinical and pathological assessment of different suture techniques for microvascular anastomosis in rat femoral artery
- PMID: 17679774
- PMCID: PMC2868134
- DOI: 10.4142/jvs.2007.8.3.269
Clinical and pathological assessment of different suture techniques for microvascular anastomosis in rat femoral artery
Abstract
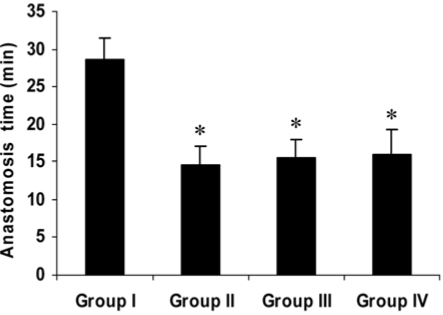
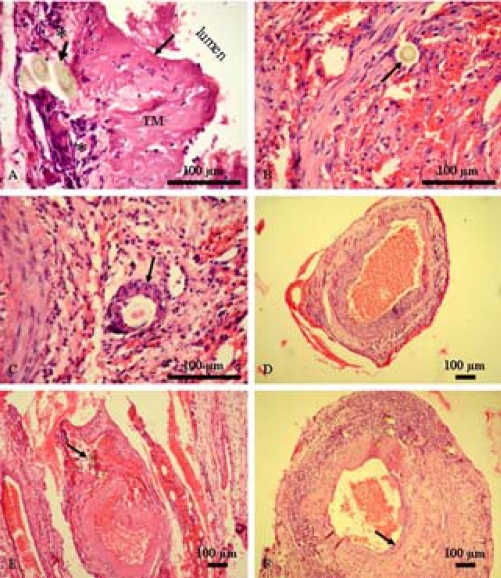
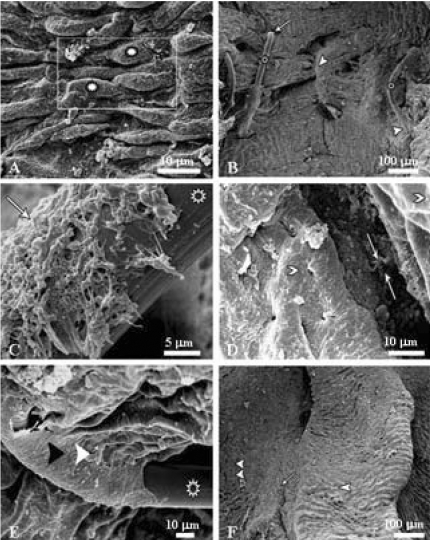
This study examined the clinical and pathological features after a microvascular anastomosis of a rat femoral artery using four different suture techniques. Sixty Sprage-Dawely rats were divided randomly into 4 groups. Fifteen bisected arteries (one from each animal) in Group I, II, III and IV were sutured with the simple interrupted suture, continuous suture, sleeve suture and cuff suture, respectively. The anastomosis times in Group I, II, III and IV were 28.67, 14.67, 15.47 and 15.93 min, respectively. Immediate bleeding that stopped without intervention (grade I) was observed in 67%, 73% and 60% of the anastomosed vessels in Groups II, III and IV, respectively, while 60% of the vessels in Group I showed light bleeding that was inhibited by gentile pressure (grade II). All vessels examined appeared to be patent at 5 and 15 min after the anastomosis. On the 7th day postoperatively, the vessels of Group I showed the highest patency rate (93%) compared with Groups II (67%), III (73%) and IV (87%). Moreover, there were more pronounced pathological changes in Group I than in the other groups. These changes included endothelial loss, endothelial proliferation, degeneration and necrosis of the tunica media. Suture materials surrounded by an inflammatory reaction were also observed. In conclusion, the simple interrupted suture is preferable for microvascular anastomosis due to its highest patency rate. The other techniques investigated can be good alternatives because of their short anastomotic time and moderate pathological changes.
Figures
Similar articles
-
Use of continuous horizontal mattress suture techniques in microsurgery: an experimental study in rats.J Hand Surg Am. 2005 May;30(3):587-95. doi: 10.1016/j.jhsa.2004.11.003. J Hand Surg Am. 2005. PMID: 15925172
-
Continuous versus interrupted suture technique in microvascular anastomosis in rats.Acta Cir Bras. 2017 Sep;32(9):691-696. doi: 10.1590/s0102-865020170090000001. Acta Cir Bras. 2017. PMID: 29019586
-
A comparison of different suture techniques for microvascular anastomosis.Ann Plast Surg. 1994 Jul;33(1):28-31. doi: 10.1097/00000637-199407000-00006. Ann Plast Surg. 1994. PMID: 7944193
-
An intraluminal stent facilitates light-activated vascular anastomosis.J Trauma Acute Care Surg. 2017 Jul;83(1 Suppl 1):S43-S49. doi: 10.1097/TA.0000000000001487. J Trauma Acute Care Surg. 2017. PMID: 28383474
-
Effect of torsion on microarterial anastomosis patency.Microsurgery. 2003;23(1):56-9. doi: 10.1002/micr.10092. Microsurgery. 2003. PMID: 12616520
Cited by
-
The "Needle-splint" Technique: A Method of Accurate Apposition and Eversion during Microvascular Anastomosis.Plast Reconstr Surg Glob Open. 2020 Jan 27;8(1):e2611. doi: 10.1097/GOX.0000000000002611. eCollection 2020 Jan. Plast Reconstr Surg Glob Open. 2020. PMID: 32095413 Free PMC article.
-
Suppression of JAK2/STAT3 signaling reduces end-to-end arterial anastomosis induced cell proliferation in common carotid arteries of rats.PLoS One. 2013;8(3):e58730. doi: 10.1371/journal.pone.0058730. Epub 2013 Mar 14. PLoS One. 2013. PMID: 23516544 Free PMC article.
-
Anterior-interrupted and posterior-continuous suture technique improved the success rate of kidney transplantation model in rats.Acta Cir Bras. 2024 Sep 20;39:e396024. doi: 10.1590/acb396024. eCollection 2024. Acta Cir Bras. 2024. PMID: 39319899 Free PMC article.
References
-
- Acland RD, Trachtenberg L. The histopathology of small arteries following experimental microvascular anastomosis. Plast Reconstr Surg. 1977;60:868–875. - PubMed
-
- Bancroft JD, Stevens A. Theory and Practice of Histological Techniques. 3rd ed. Edinburgh: Churchill Livingstone; 1990. pp. 113–305.
-
- Chen YX, Chen LE, Seaber AV, Urbaniak JR. Comparison of continuous and interrupted suture techniques in microvascular anastomosis. J Hand Surg [AM] 2001;26:530–539. - PubMed
-
- Ching S, Thoma A, Monkman S, Kelton JG. Inhibition of microsurgical thrombosis by the platelet glycoprotein IIb/IIIa antagonist SR121566A. Plast Reconstr Surg. 2003;112:177–185. - PubMed
-
- Cobbett J. Small vessel anastomosis. A comparison of suture techniques. Br J Plast Surg. 1967;20:16–20. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
