

Health care-associated pneumonia and community-acquired pneumonia: a single-center experience
- PMID: 17682100
- PMCID: PMC2043297
- DOI: 10.1128/AAC.00851-07
Health care-associated pneumonia and community-acquired pneumonia: a single-center experience
Abstract
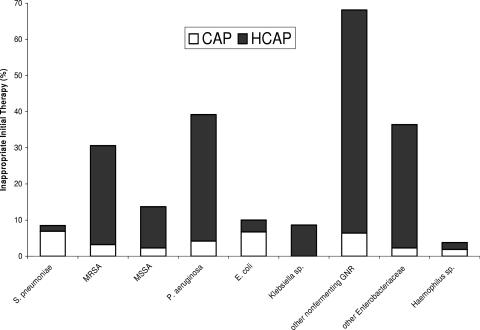
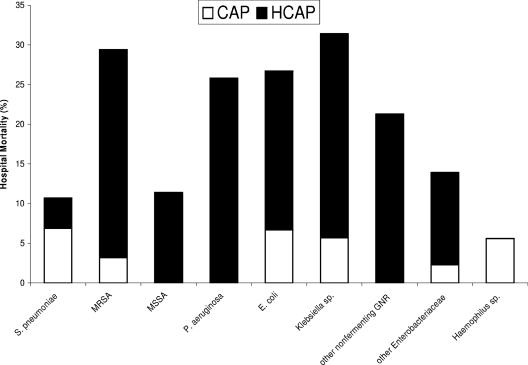
Pneumonia occurring outside of the hospital setting has traditionally been categorized as community-acquired pneumonia (CAP). However, when pneumonia is associated with health care risk factors (prior hospitalization, dialysis, residing in a nursing home, immunocompromised state), it is now more appropriately classified as a health care-associated pneumonia (HCAP). The relative incidences of CAP and HCAP among patients requiring hospital admission is not well described. The objective of this retrospective cohort study, involving 639 patients with culture-positive CAP and HCAP admitted between 1 January 2003 and 31 December 2005, was to characterize the incidences, microbiology, and treatment patterns for CAP and HCAP among patients requiring hospital admission. HCAP was more common than CAP (67.4% versus 32.6%). The most common pathogens identified overall included methicillin-resistant Staphylococcus aureus (24.6%), Streptococcus pneumoniae (20.3%), Pseudomonas aeruginosa (18.8%), methicillin-sensitive Staphylococcus aureus (13.8%), and Haemophilus influenzae (8.5%). The hospital mortality rate was statistically greater among patients with HCAP than among those with CAP (24.6% versus 9.1%; P < 0.001). Administration of inappropriate initial antimicrobial treatment was statistically more common among HCAP patients (28.3% versus 13.0%; P < 0.001) and was identified as an independent risk factor for hospital mortality. Our study found that the incidence of HCAP was greater than that of CAP among patients with culture-positive pneumonia requiring hospitalization at Barnes-Jewish Hospital. Patients with HCAP were more likely to initially receive inappropriate antimicrobial treatment and had a greater risk of hospital mortality. Health care providers should differentiate patients with HCAP from those with CAP in order to provide more appropriate initial antimicrobial therapy.
Figures
References
-
- Alvarez-Lerma, F. 1996. Modification of empiric antibiotic treatment in patients with pneumonia acquired in the intensive care unit. Intensive Care Med. 22:387-394. - PubMed
-
- Garnacho-Montero, J., J. L. Garcia-Garmendia, A. Barrero-Almodovar, F. J. Jimenez-Jimenez, C. Perez-Paredes, and C. Ortiz-Leyba. 2003. Impact of adequate empirical antibiotic therapy on the outcome of patients admitted to the intensive care unit with sepsis. Crit. Care Med. 31:2742-2751. - PubMed
-
- Harbarth, S., K. Ferriere, S. Hugonnet, B. Ricou, P. Suter, and D. Pittet. 2002. Epidemiology and prognostic determinants of bloodstream infections in surgical intensive care. Arch. Surg. 137:1353-1359. - PubMed
-
- Harbarth, S., J. Garbino, J. Pugin, J. A. Romand, D. Lew, and D. Pittet. 2003. Inappropriate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis. Am. J. Med. 115:529-535. - PubMed
-
- Hospital-Acquired Pneumonia Guideline Committee of the American Thoracic Society and Infectious Diseases Society of America. 2005. Guidelines for the management of adults with hospital-acquired pneumonia, ventilator-associated pneumonia, and healthcare-associated pneumonia. Am. J. Respir. Crit. Care Med. 171:388-416. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
