

Applying psychological theories to evidence-based clinical practice: identifying factors predictive of managing upper respiratory tract infections without antibiotics
- PMID: 17683558
- PMCID: PMC2042498
- DOI: 10.1186/1748-5908-2-26
Applying psychological theories to evidence-based clinical practice: identifying factors predictive of managing upper respiratory tract infections without antibiotics
Abstract
Background: Psychological models can be used to understand and predict behaviour in a wide range of settings. However, they have not been consistently applied to health professional behaviours, and the contribution of differing theories is not clear. The aim of this study was to explore the usefulness of a range of psychological theories to predict health professional behaviour relating to management of upper respiratory tract infections (URTIs) without antibiotics.
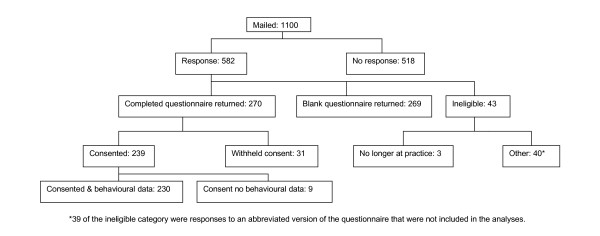
Methods: Psychological measures were collected by postal questionnaire survey from a random sample of general practitioners (GPs) in Scotland. The outcome measures were clinical behaviour (using antibiotic prescription rates as a proxy indicator), behavioural simulation (scenario-based decisions to managing URTI with or without antibiotics) and behavioural intention (general intention to managing URTI without antibiotics). Explanatory variables were the constructs within the following theories: Theory of Planned Behaviour (TPB), Social Cognitive Theory (SCT), Common Sense Self-Regulation Model (CS-SRM), Operant Learning Theory (OLT), Implementation Intention (II), Stage Model (SM), and knowledge (a non-theoretical construct). For each outcome measure, multiple regression analysis was used to examine the predictive value of each theoretical model individually. Following this 'theory level' analysis, a 'cross theory' analysis was conducted to investigate the combined predictive value of all significant individual constructs across theories.
Results: All theories were tested, but only significant results are presented. When predicting behaviour, at the theory level, OLT explained 6% of the variance and, in a cross theory analysis, OLT 'evidence of habitual behaviour' also explained 6%. When predicting behavioural simulation, at the theory level, the proportion of variance explained was: TPB, 31%; SCT, 26%; II, 6%; OLT, 24%. GPs who reported having already decided to change their management to try to avoid the use of antibiotics made significantly fewer scenario-based decisions to prescribe. In the cross theory analysis, perceived behavioural control (TPB), evidence of habitual behaviour (OLT), CS-SRM cause (chance/bad luck), and intention entered the equation, together explaining 36% of the variance. When predicting intention, at the theory level, the proportion of variance explained was: TPB, 30%; SCT, 29%; CS-SRM 27%; OLT, 43%. GPs who reported that they had already decided to change their management to try to avoid the use of antibiotics had a significantly higher intention to manage URTIs without prescribing antibiotics. In the cross theory analysis, OLT evidence of habitual behaviour, TPB attitudes, risk perception, CS-SRM control by doctor, TPB perceived behavioural control and CS-SRM control by treatment entered the equation, together explaining 49% of the variance in intention.
Conclusion: The study provides evidence that psychological models can be useful in understanding and predicting clinical behaviour. Taking a theory-based approach enables the creation of a replicable methodology for identifying factors that predict clinical behaviour. However, a number of conceptual and methodological challenges remain.
References
-
- McCormick A, Fleming D, Charlton J. Morbidity statistics from general practice Fourth national study 1991-1992. London, OPCS, HMSO; 1995.
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
