

Modern perspectives in the treatment of chronic anal fissures
- PMID: 17688717
- PMCID: PMC2048592
- DOI: 10.1308/003588407X202137
Modern perspectives in the treatment of chronic anal fissures
Abstract
Introduction: Anal fissures are commonly encountered in routine colorectal practice. Developments in the pharmacological understanding of the internal anal sphincter have resulted in more conservative approaches towards treatment. Simple measures are often effective for early fissures. Glyceryl trinitrate is well established as a first-line pharmacological therapy. The roles of diltiazem and botulinum, particularly as rescue therapy, are not well understood. Surgery has a defined role and should not be discounted completely.
Methods: Data were obtained from Medline publications citing 'anal fissure'. Manual cross-referencing of salient articles was conducted. We have sought to highlight various controversies in the management of anal fissures.
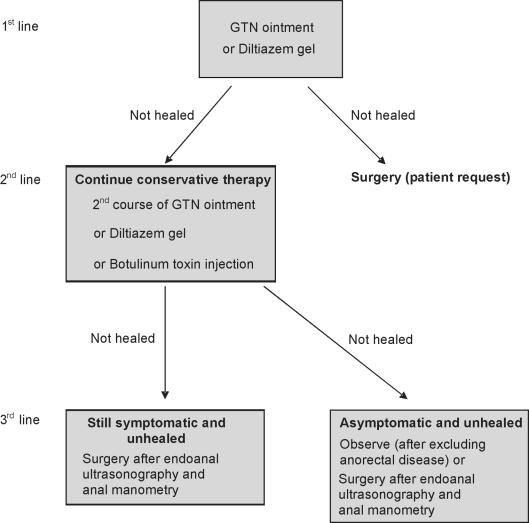
Findings: Acute fissures may heal spontaneously, although simple conservative measures are sufficient. Idiopathic chronic anal fissures need careful evaluation to decide what therapy is suitable. Pharmacological agents such as glyceryl trinitrate (GTN), diltiazem and botulinum toxin have been subjected to most scrutiny. Though practices in the UK vary, GTN or diltiazem would be suitable as first-line therapy with botulinum toxin used as rescue treatment. Sphincterotomy is indicated for unhealed fissures; fissurectomy has been revisited and advancement flaps have a role in patients in whom sphincter division is not suitable.
Figures
Similar articles
-
Botulinum toxin as second-line therapy for chronic anal fissure failing 0.2 percent glyceryl trinitrate.Dis Colon Rectum. 2003 Mar;46(3):361-6. doi: 10.1007/s10350-004-6556-7. Dis Colon Rectum. 2003. PMID: 12626912 Clinical Trial.
-
Progress in the understanding and treatment of chronic anal fissure.Postgrad Med J. 2001 Dec;77(914):753-8. doi: 10.1136/pmj.77.914.753. Postgrad Med J. 2001. PMID: 11723312 Free PMC article. Review.
-
Chemical sphincterotomy--first line of treatment for chronic anal fissure.Mymensingh Med J. 2005 Jan;14(1):88-90. Mymensingh Med J. 2005. PMID: 15695964 Review.
-
Partial lateral internal sphincterotomy versus combined botulinum toxin A injection and topical diltiazem in the treatment of chronic anal fissure: a randomized clinical trial.Dis Colon Rectum. 2015 Feb;58(2):228-34. doi: 10.1097/DCR.0000000000000307. Dis Colon Rectum. 2015. PMID: 25585082 Clinical Trial.
-
Randomized clinical trial of botulinum toxin plus glyceryl trinitrate vs. botulinum toxin alone for medically resistant chronic anal fissure: overall poor healing rates.Dis Colon Rectum. 2006 Oct;49(10):1574-80. doi: 10.1007/s10350-006-0679-y. Dis Colon Rectum. 2006. PMID: 16988850 Clinical Trial.
Cited by
-
Beyond Beauty : Botulinum Toxin Use in Anal Fissure.Med J Armed Forces India. 2009 Jul;65(3):213-5. doi: 10.1016/S0377-1237(09)80005-1. Epub 2011 Jul 21. Med J Armed Forces India. 2009. PMID: 27408248 Free PMC article.
-
The management of patients with primary chronic anal fissure: a position paper.Tech Coloproctol. 2011 Jun;15(2):135-41. doi: 10.1007/s10151-011-0683-7. Epub 2011 May 3. Tech Coloproctol. 2011. PMID: 21538013 Free PMC article. Review.
-
Effect of chronic anal fissure components on isosorbide dinitrate treatment.World J Surg. 2012 Sep;36(9):2225-9. doi: 10.1007/s00268-012-1604-2. World J Surg. 2012. PMID: 22526048
-
Glyceryl trinitrate ointment did not reduce pain after stapled hemorrhoidectomy: a randomized controlled trial.Int Surg. 2012 Apr-Jun;97(2):112-9. doi: 10.9738/CC92.1. Int Surg. 2012. PMID: 23102076 Free PMC article. Clinical Trial.
-
A Comparative Study of Lateral Sphincterotomy and 2% Diltiazem Gel Local Application in the Treatment of Chronic Fissure in ANO.J Clin Diagn Res. 2014 Oct;8(10):NC01-2. doi: 10.7860/JCDR/2014/10480.4925. Epub 2014 Oct 20. J Clin Diagn Res. 2014. PMID: 25478389 Free PMC article.
References
-
- Sharp FR. Patient selection and treatment modalities for chronic anal fissure. Am J Surg. 1996;171:512–5. - PubMed
-
- McDonald P, Driscoll AM, Nicholls RJ. The anal dilator in the conservative management of acute anal fissures. Br J Surg. 1983;70:25–6. - PubMed
-
- Shub HA, Salvati EP, Rubin RJ. Conservative treatment of anal fissure: an unselected, retrospective and continuous study. Dis Colon Rectum. 1978;21:582–3. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources