

Health locus of control and use of conventional and alternative care: a cohort study
- PMID: 17688759
- PMCID: PMC2099670
Health locus of control and use of conventional and alternative care: a cohort study
Abstract
Background: Health locus of control influences health-related behaviour, but its association with healthcare use is unclear.
Aim: To investigate the association between individuals' health locus of control and the use of conventional and alternative health care.
Design of study: Prospective cohort study.
Setting: A nationally representative random sample of community-dwelling adult households in Japan.
Method: Health locus of control, symptom-related visits to physicians, and the use of dietary and physical complementary and alternative medicine (CAM) was measured. Dietary CAM included supplements, such as herbs and vitamins. Physical CAM included manipulations, such as acupuncture and acupressure.
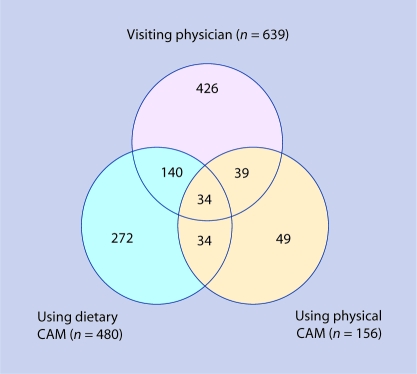
Results: Of the 2453 adult participants studied, 2103 (86%; 95% CI [confidence interval] = 84 to 88%) developed at least one symptom during the 31-day study period. Of these symptomatic adults, 639 visited physicians (30%; 95% CI = 28 to 32%), 480 used dietary CAM (23%; 95% CI = 21 to 25%), and 156 (7%; 95% CI = 6 to 9%) used physical CAM. The likelihood of visiting a physician was not related significantly to individuals' health locus of control. Increased use of dietary CAM was weakly associated with control by spiritual powers (P = 0.028), internal control (P = 0.013), and less control by professionals (P = 0.020). Increased use of physical CAM was significantly associated with control by spiritual powers (P = 0.009) indicating a belief that supernatural forces control individuals' health status.
Conclusion: The likelihood of visiting a physician is not affected by individuals' health locus of control. Control by spiritual powers is involved with increased CAM use. Internal control is weakly associated with greater use of dietary CAM; professional control is weakly associated with less use of dietary CAM.
Figures
Similar articles
-
Sex differences in motives for use of complementary and alternative medicine among cancer patients.Altern Ther Health Med. 2004 Sep-Oct;10(5):58-64. Altern Ther Health Med. 2004. PMID: 15478787
-
Higher internality of health locus of control is associated with the use of complementary and alternative medicine providers among patients seeking care for acute low-back pain.Clin J Pain. 2008 Oct;24(8):725-30. doi: 10.1097/AJP.0b013e3181759261. Clin J Pain. 2008. PMID: 18806538
-
Factors influencing the use of complementary and alternative medicine and whether patients inform their primary care physician.Complement Ther Med. 2012 Feb-Apr;20(1-2):45-53. doi: 10.1016/j.ctim.2011.10.001. Epub 2011 Nov 3. Complement Ther Med. 2012. PMID: 22305248
-
Provider-based complementary and alternative medicine use among three chronic illness groups: associations with psychosocial factors and concurrent use of conventional health-care services.Complement Ther Med. 2008 Apr;16(2):73-80. doi: 10.1016/j.ctim.2007.03.006. Epub 2007 Jun 6. Complement Ther Med. 2008. PMID: 18514908
-
Perceptions and attitudes of rehabilitation medicine physicians on complementary and alternative medicine in Australia.Intern Med J. 2009 Mar;39(3):164-9. doi: 10.1111/j.1445-5994.2008.01734.x. Intern Med J. 2009. PMID: 19383065
Cited by
-
Opinions on Kampo and reasons for using it--results from a cross-sectional survey in three Japanese clinics.BMC Complement Altern Med. 2013 May 16;13:108. doi: 10.1186/1472-6882-13-108. BMC Complement Altern Med. 2013. PMID: 23680097 Free PMC article.
-
Traditional and complementary medicine for promoting healthy ageing in WHO Western Pacific Region: Policy implications from utilization patterns and current evidence.Integr Med Res. 2021 Mar;10(1):100469. doi: 10.1016/j.imr.2020.100469. Epub 2020 Jul 4. Integr Med Res. 2021. PMID: 32874912 Free PMC article. Review.
-
Demographics, health literacy and health locus of control beliefs of Australian women who take complementary medicine products during pregnancy and breastfeeding: A cross-sectional, online, national survey.Health Expect. 2022 Apr;25(2):667-683. doi: 10.1111/hex.13414. Epub 2021 Dec 23. Health Expect. 2022. PMID: 34951097 Free PMC article.
References
-
- Wallston BS, Wallston KA, Kaplan GD, Maides SA. Development and validation of the health locus of control (HLC) scale. J Consult Clin Psychol. 1976;44(4):580–585. - PubMed
-
- Wallston KA, Wallston BS, DeVellis R. Development of the multidimensional health locus of control (MHLC) scales. Health Educ Monogr. 1978;6(2):160–170. - PubMed
-
- Wallston KA. The validity of the multidimensional health locus of control scales. J Health Psychol. 2005;10(5):623–631. - PubMed
-
- Kuwahara A, Nishino Y, Ohkubo T, et al. Reliability and validity of the multidimensional health locus of control scale in Japan: relationship with demographic factors and health-related behaviour. Tohoku J Exp Med. 2004;203(1):37–45. - PubMed
-
- Yoshida Y, Takagi H, Inaba Y. [Health locus of control and acquisition of health-related information] Nippon Koshu Eisei Zasshi. 1995;42(2):69–77. (In Japanese.) - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials