

Targeting TNFalpha rapidly reduces density of dendritic cells and macrophages in psoriatic plaques with restoration of epidermal keratinocyte differentiation
- PMID: 17689932
- PMCID: PMC2703191
- DOI: 10.1016/j.jdermsci.2007.06.006
Targeting TNFalpha rapidly reduces density of dendritic cells and macrophages in psoriatic plaques with restoration of epidermal keratinocyte differentiation
Abstract
Background: The cytokine network theory for psoriasis postulates a key role for TNFalpha in mediating inflammation and altered epidermal differentiation.
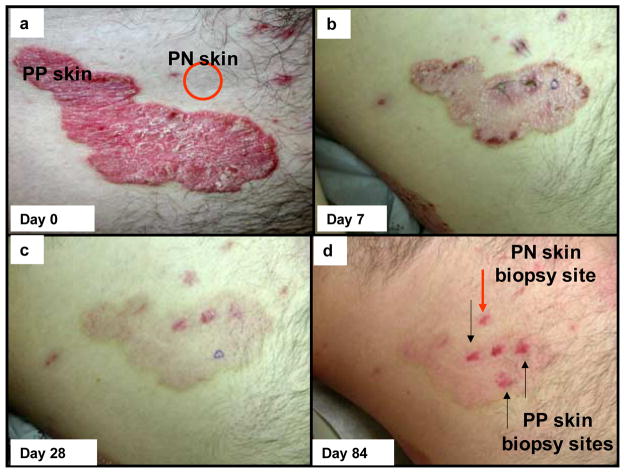
Objective: This study defines responses following administration of adalimumab, a TNFalpha inhibitor, in pre-psoriatic skin (PN) and lesional psoriatic plaques (PP) skin.
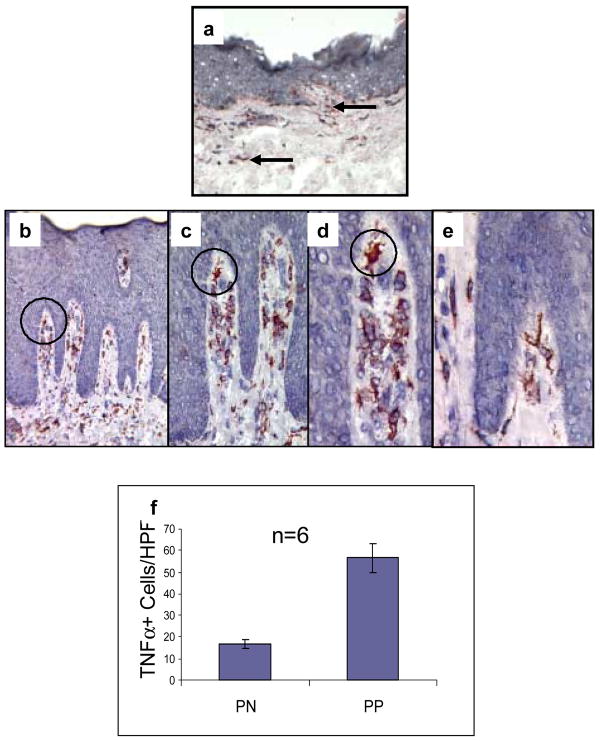
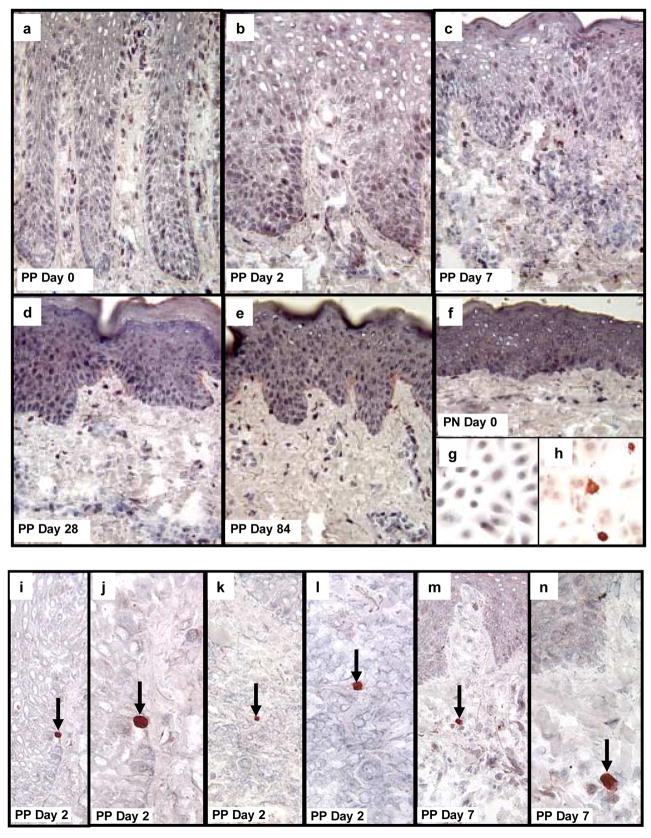
Methods: PN and PP skin before and after treatment were biopsied at days 2, 7, 28 and 84 (n=6 different patients). Cryosections were immunohistochemically stained to detect TNFalpha and other relevant markers in epidermal and dermal compartments. Detection of apoptosis utilized antibody specific for activated caspase 3. Semiquantitative assessments and statistical analysis was performed for each staining profile.
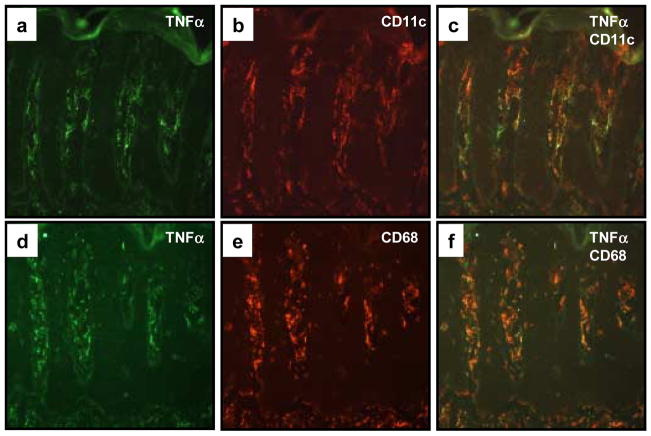
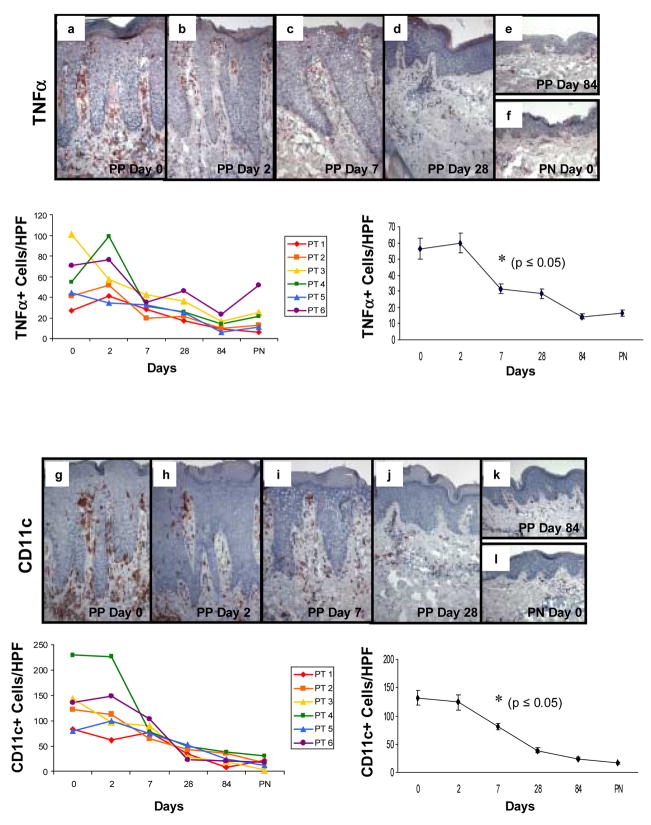
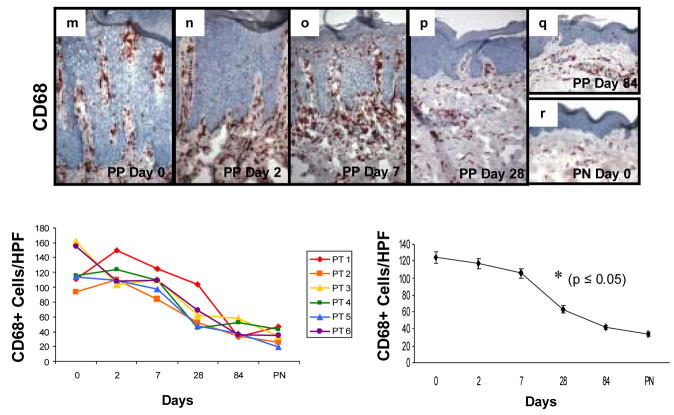
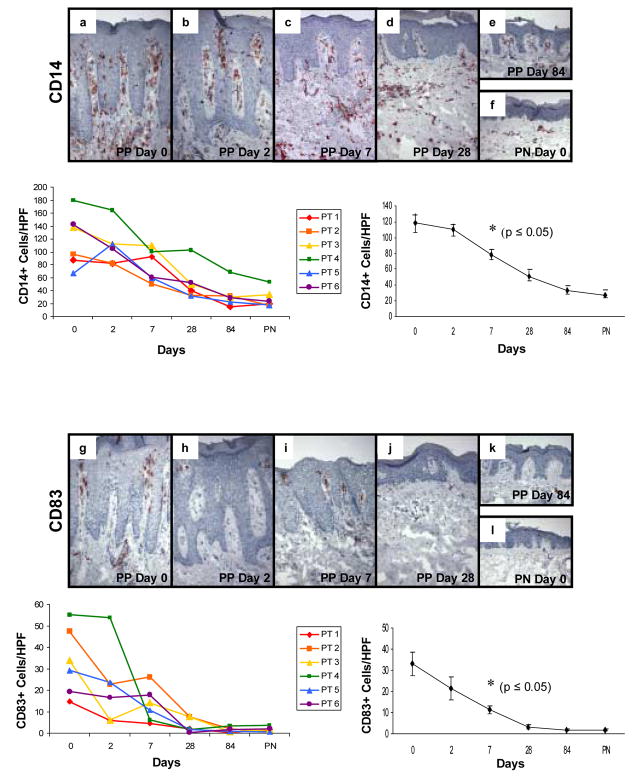
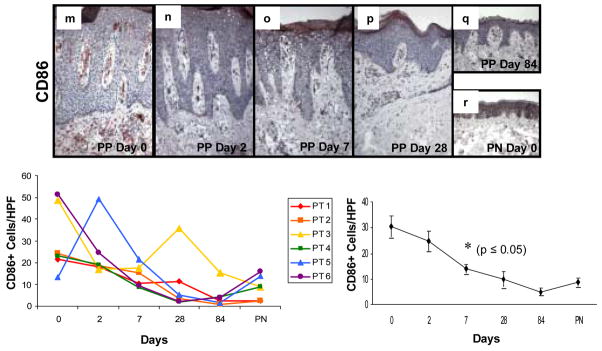
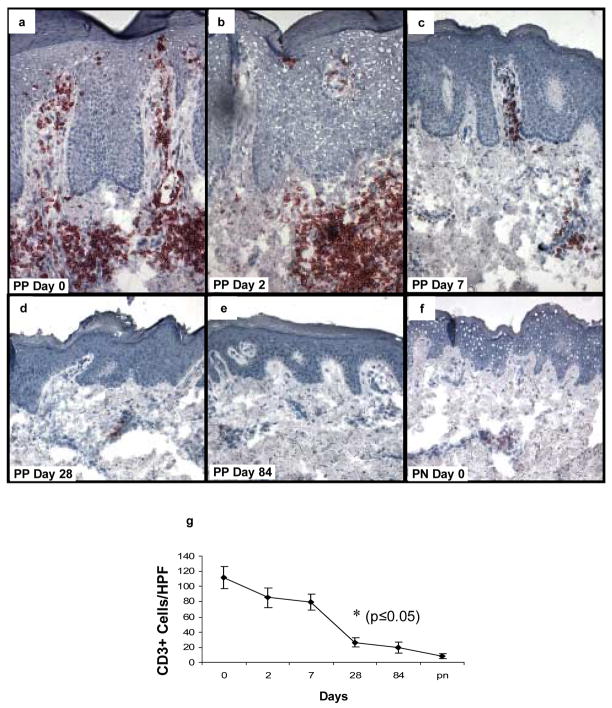
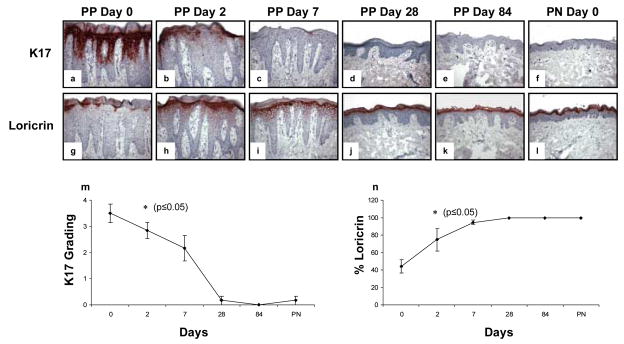
Results: TNFalpha+ cells were increased in PP skin. PP skin was also characterized by a four-fold increase in number of CD68+ macrophages as well as eight-fold increase in CD11c+ dermal dendritic cells (DCs) compared to PN skin. By two-color immunofluorescence staining, both CD68+ cells as well as CD11c+ cells expressed TNFalpha. Following initiation of adalimumab therapy, CD11c+ cells, significantly decreased in PP skin at days 7, 28, and 84, while CD68+ and CD14+ cells decreased at days 28 and 84. Other markers for DCs (CD83, CD86) showed decreases at days 7, 28, and 84. Reduction in DCs, macrophages or T cells was not accompanied by increased activated caspase 3-positive cells. When a keratinocyte terminal differentiation marker was examined, adalimumab triggered rapid restoration of loricrin expression (beginning on day 2), with loss of aberrant differentiation marker, keratin 17 (K17).
Conclusion: Adalimumab impacts dermal-based immunocytes, and the epidermal compartment also responds by restoration of normal differentiation without detectable apoptosis.
Figures
Similar articles
-
The tumour necrosis factor-alpha inhibitor adalimumab rapidly reverses the decrease in epidermal Langerhans cell density in psoriatic plaques.Br J Dermatol. 2005 Nov;153(5):945-53. doi: 10.1111/j.1365-2133.2005.06816.x. Br J Dermatol. 2005. PMID: 16225604 Clinical Trial.
-
Preferential inhibition of the mRNA expression of p38 mitogen-activated protein kinase regulated cytokines in psoriatic skin by anti-TNFα therapy.Br J Dermatol. 2010 Dec;163(6):1194-204. doi: 10.1111/j.1365-2133.2010.10036.x. Br J Dermatol. 2010. PMID: 20846304
-
Early effects of tumour necrosis factor alpha blockade on skin and synovial tissue in patients with active psoriasis and psoriatic arthritis.Ann Rheum Dis. 2004 Jul;63(7):769-73. doi: 10.1136/ard.2003.018085. Ann Rheum Dis. 2004. PMID: 15194570 Free PMC article. Clinical Trial.
-
Tumor necrosis factor-alpha inhibitor-induced psoriasis or psoriasiform exanthemata: first 120 cases from the literature including a series of six new patients.Am J Clin Dermatol. 2008;9(1):1-14. doi: 10.2165/00128071-200809010-00001. Am J Clin Dermatol. 2008. PMID: 18092839 Review.
-
Adalimumab for the treatment of severe psoriasis and psoriatic arthritis.Expert Opin Biol Ther. 2008 Mar;8(3):363-70. doi: 10.1517/14712598.8.3.363. Expert Opin Biol Ther. 2008. PMID: 18294106 Review.
Cited by
-
Macrophages in dermatology: pathogenic roles and targeted therapeutics.Arch Dermatol Res. 2022 Mar;314(2):133-140. doi: 10.1007/s00403-021-02207-0. Epub 2021 Feb 28. Arch Dermatol Res. 2022. PMID: 33641015 Review.
-
Single-cell RNA-Seq reveals the transcriptional landscape and heterogeneity of skin macrophages in Vsir-/- murine psoriasis.Theranostics. 2020 Aug 21;10(23):10483-10497. doi: 10.7150/thno.45614. eCollection 2020. Theranostics. 2020. PMID: 32929361 Free PMC article.
-
Semaphorin 3A: A potential target for prevention and treatment of nickel allergy.Commun Biol. 2022 Jul 7;5(1):671. doi: 10.1038/s42003-022-03641-0. Commun Biol. 2022. PMID: 35798870 Free PMC article.
-
NETosis of psoriasis: a critical step in amplifying the inflammatory response.Front Immunol. 2024 Aug 1;15:1374934. doi: 10.3389/fimmu.2024.1374934. eCollection 2024. Front Immunol. 2024. PMID: 39148738 Free PMC article. Review.
-
CD169+ Skin Macrophages Function as a Specialized Subpopulation in Promoting Psoriasis-like Skin Disease in Mice.Int J Mol Sci. 2024 May 24;25(11):5705. doi: 10.3390/ijms25115705. Int J Mol Sci. 2024. PMID: 38891893 Free PMC article.
References
-
- Krueger JG. The immunologic basis for the treatment of psoriasis with new biologic agents. J Am Acad Dermatol. 2002;46:1–23. - PubMed
-
- McKay IA, Leigh IM. Altered keratinocyte growth and differentiation in psoriasis. Clin Dermatol. 1995;13:105–114. - PubMed
-
- Austin LM, Ozawa M, Kikuchi T, Walters IB, Krueger JG. The majority of epidermal T cells in Psoriasis vulgaris lesions can produce type 1 cytokines, interferon-gamma, interleukin-2, and tumor necrosis factor-alpha, defining TC1 (cytotoxic T lymphocyte) and TH1 effector populations: a type 1 differentiation bias is also measured in circulating blood T cells in psoriatic patients. J Invest Dermatol. 1999;113:752–759. - PubMed
-
- Lew W, Bowcock AM, Krueger JG. Psoriasis vulgaris: cutaneous lymphoid tissue supports T-cell activation and “Type 1” inflammatory gene expression. Trends Immunol. 2004;25:295–305. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
