

Eliminating human tuberculosis in the twenty-first century
- PMID: 17690054
- PMCID: PMC3226985
- DOI: 10.1098/rsif.2007.1138
Eliminating human tuberculosis in the twenty-first century
Abstract
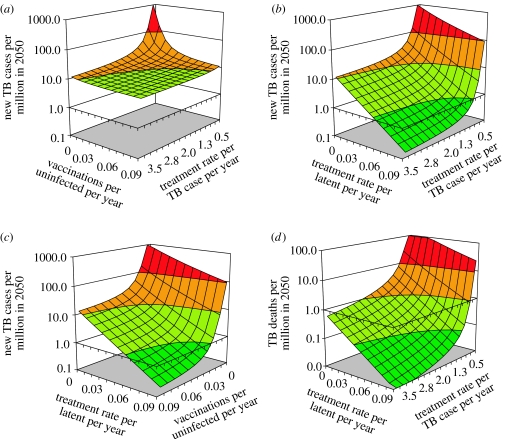
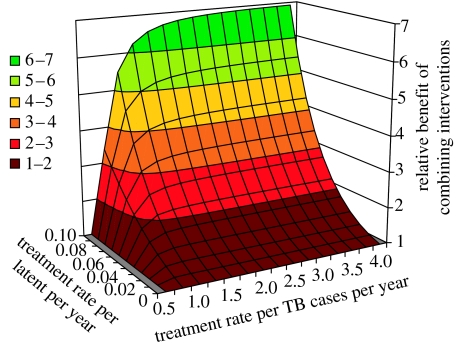
Recognizing that tuberculosis (TB) is still the leading cause of human death from a curable infection, the international health community has set ambitious targets for disease control. One target is to eliminate TB by 2050; that is, to cut the annual incidence of new cases to less than 1 per million population. National TB control programmes are working to eliminate TB mainly by intensifying efforts to find and cure patients with active disease. Here, we use mathematical modelling to show that, while most TB patients can be cured with present drug regimens, the 2050 target is far more likely to be achieved with a combination of diagnostics, drugs and vaccines that can detect and treat both latent infection and active disease. We find that the coupling of control methods is particularly effective because treatments for latent infection and active disease act in synergy. This synergistic effect offers new perspectives on the cost-effectiveness of treating latent TB infection and the impact of possible new TB vaccines. Our results should be a stimulus to those who develop, manufacture and implement new technology for TB control, and to their financial donors.
Figures

References
-
- Anderson R.M, May R.M. Oxford University Press; Oxford, UK: 1991. Infectious diseases of humans: dynamics and control.
-
- Berkeley Madonna. Berkeley-Madonna: modeling and analysis of dynamic systems. University of California; Berkeley, CA: 2007.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical