

The impact of a closed-loop electronic prescribing and administration system on prescribing errors, administration errors and staff time: a before-and-after study
- PMID: 17693676
- PMCID: PMC2464943
- DOI: 10.1136/qshc.2006.019497
The impact of a closed-loop electronic prescribing and administration system on prescribing errors, administration errors and staff time: a before-and-after study
Abstract
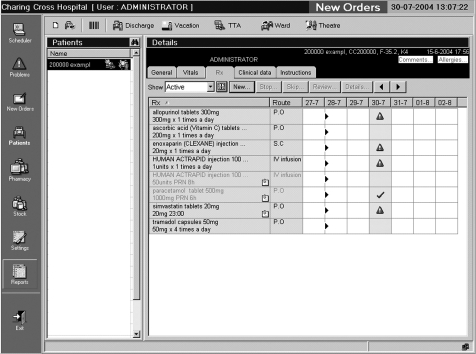
Objectives: To assess the impact of a closed-loop electronic prescribing, automated dispensing, barcode patient identification and electronic medication administration record (EMAR) system on prescribing and administration errors, confirmation of patient identity before administration, and staff time.
Design, setting and participants: Before-and-after study in a surgical ward of a teaching hospital, involving patients and staff of that ward.
Intervention: Closed-loop electronic prescribing, automated dispensing, barcode patient identification and EMAR system.
Main outcome measures: Percentage of new medication orders with a prescribing error, percentage of doses with medication administration errors (MAEs) and percentage given without checking patient identity. Time spent prescribing and providing a ward pharmacy service. Nursing time on medication tasks.
Results: Prescribing errors were identified in 3.8% of 2450 medication orders pre-intervention and 2.0% of 2353 orders afterwards (p<0.001; chi(2) test). MAEs occurred in 7.0% of 1473 non-intravenous doses pre-intervention and 4.3% of 1139 afterwards (p = 0.005; chi(2) test). Patient identity was not checked for 82.6% of 1344 doses pre-intervention and 18.9% of 1291 afterwards (p<0.001; chi(2) test). Medical staff required 15 s to prescribe a regular inpatient drug pre-intervention and 39 s afterwards (p = 0.03; t test). Time spent providing a ward pharmacy service increased from 68 min to 98 min each weekday (p = 0.001; t test); 22% of drug charts were unavailable pre-intervention. Time per drug administration round decreased from 50 min to 40 min (p = 0.006; t test); nursing time on medication tasks outside of drug rounds increased from 21.1% to 28.7% (p = 0.006; chi(2) test).
Conclusions: A closed-loop electronic prescribing, dispensing and barcode patient identification system reduced prescribing errors and MAEs, and increased confirmation of patient identity before administration. Time spent on medication-related tasks increased.
Conflict of interest statement
Competing interests: The authors' work was independent of MDG Medical.


Similar articles
-
The impact of closed-loop electronic medication management on time to first dose: a comparative study between paper and digital hospital environments.Int J Pharm Pract. 2018 Dec;26(6):526-533. doi: 10.1111/ijpp.12432. Epub 2018 Jan 22. Int J Pharm Pract. 2018. PMID: 29356171
-
Qualitative evaluation of an electronic prescribing and administration system.Qual Saf Health Care. 2007 Aug;16(4):271-8. doi: 10.1136/qshc.2006.019505. Qual Saf Health Care. 2007. PMID: 17693675 Free PMC article.
-
Influence of computerised medication charts on medication errors in a hospital.Drug Saf. 2005;28(12):1119-29. doi: 10.2165/00002018-200528120-00006. Drug Saf. 2005. PMID: 16329714
-
Errors in medicine administration: how can they be minimised?J Perioper Pract. 2008 Jun;18(6):249-53. doi: 10.1177/175045890801800604. J Perioper Pract. 2008. PMID: 18616203 Review.
-
Safety, time and cost evaluation of automated and semi-automated drug distribution systems in hospitals: a systematic review.Eur J Hosp Pharm. 2020 Sep;27(5):253-262. doi: 10.1136/ejhpharm-2018-001791. Epub 2019 Mar 19. Eur J Hosp Pharm. 2020. PMID: 32839256 Free PMC article.
Cited by
-
Technologies to reduce errors in dispensing and administration of medication in hospitals: clinical and economic analyses.CADTH Technol Overv. 2010;1(3):e0116. Epub 2010 Sep 1. CADTH Technol Overv. 2010. PMID: 22977406 Free PMC article. No abstract available.
-
The impact of a novel medication scanner on administration errors in the hospital setting: a before and after feasibility study.BMC Med Inform Decis Mak. 2022 Mar 29;22(1):86. doi: 10.1186/s12911-022-01828-3. BMC Med Inform Decis Mak. 2022. PMID: 35351096 Free PMC article.
-
Pharmacists and health information technology: emerging issues in patient safety.HEC Forum. 2008 Sep;20(3):259-75. doi: 10.1007/s10730-008-9075-4. HEC Forum. 2008. PMID: 18803019 No abstract available.
-
Position paper on patient safety.Eur J Hosp Pharm. 2020 Dec 18;28(3):129-32. doi: 10.1136/ejhpharm-2019-001924. Online ahead of print. Eur J Hosp Pharm. 2020. PMID: 33355293 Free PMC article. Review. No abstract available.
-
Drug administration errors in hospital inpatients: a systematic review.PLoS One. 2013 Jun 20;8(6):e68856. doi: 10.1371/journal.pone.0068856. Print 2013. PLoS One. 2013. PMID: 23818992 Free PMC article.
References
-
- Committee on Quality of Health Care in America, Institute of Medicine To err is human: building a safer health system. Washington, DC: National Academy Press, 2000
-
- Department of Health Building a safer NHS for patients: improving medication safety. London: Department of Health, 2004
-
- Audit Commission A spoonful of sugar—medicines management in NHS hospitals. London: Audit Commission, 2001
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical