

Guidelines in context of evidence
- PMID: 17693681
- PMCID: PMC2464948
- DOI: 10.1136/qshc.2006.019752
Guidelines in context of evidence
Abstract
Objective: In clinical practice guidelines, the quality of the available evidence is graded according to its reliability and quality. This study aimed to evaluate the quality of the available research evidence, using the levels of evidence, in the evidence summaries of 64 Finnish national evidence-based Current Care guidelines.
Design: Descriptive assessment.
Setting: Electronic web-based guidelines in Finland.
Main outcome measures: The proportions of evidence summaries with different levels of evidence (A-D).
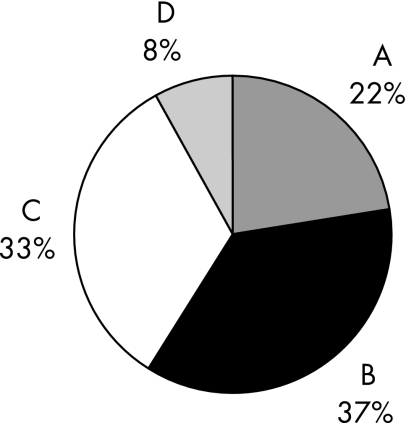
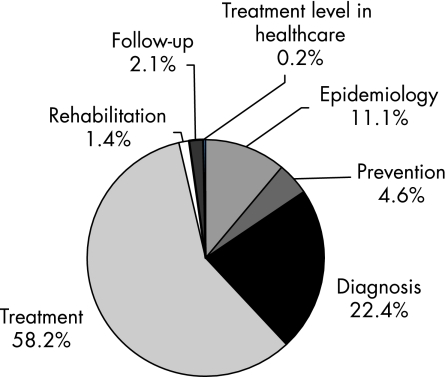
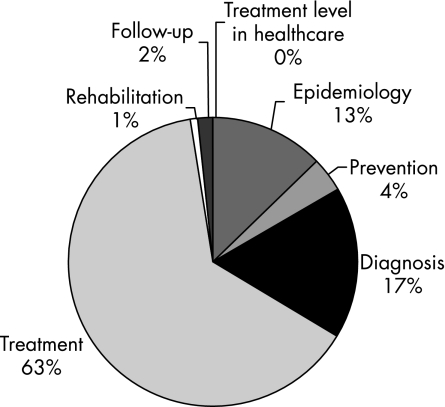
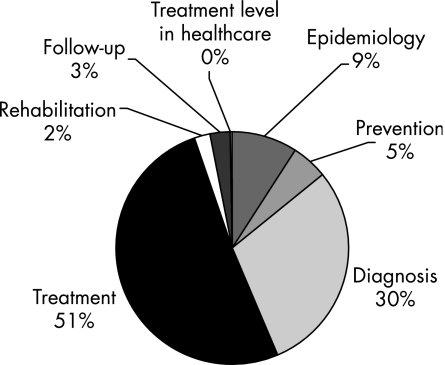
Results: The 64 guidelines had a total of 2419 evidence summaries. Of these, 532 (22.0%) were evidence level A, 891 (36.8%) were evidence level B, 808 (33.4%) were evidence level C, and 188 (7.8%) were evidence level D. Most--that is, 81% of the level C and D evidence summaries dealt with diagnosis and treatment. Most of the evidence summaries pertained to treatment (58.2%) and diagnosis (22.4%). The sections on diagnosis and treatment represented 80% of all the level A and level B evidence, and 81% of all the level C and level D evidence.
Conclusions: There is adequate high-quality evidence (level A) to support only a fifth of the main statements of the 64 guidelines. This is most likely an optimistic estimate, since level D evidence often does not have an evidence summary. The guideline development groups find it easier to agree on recommendations based on level A and level B evidence.
Conflict of interest statement
Competing interests: None.
References
-
- Shojania K G, Mcdonald K M, Wachter R M.et alClosing the quality gap: a critical analysis of quality improvement strategies, volume 1—series overview and methodology. AHRQ Publication No. 04‐0051‐1. Rockville, MD: Agency for Healthcare Research and Quality, August 2004. http://www.ahrq.gov/downloads/pub/evidence/pdf/qualgap1/qualgap1.pdf (accessed 3 June 2006) - PubMed
-
- Staniszewska S H, Henderson L. Patients' evaluations of the quality of care: influencing factors and the importance of engagement. J Adv Nurs 200549530–537. - PubMed
-
- Muir Gray J A.Evidence‐based health care: how to make health policy and management decisions. Edinburgh: Churchill Livingstone, 2001
MeSH terms
LinkOut - more resources
Full Text Sources