

Assessment of T staging and mesorectal fascia status using high-resolution MRI in rectal cancer with rectal distention
- PMID: 17696238
- PMCID: PMC4205321
- DOI: 10.3748/wjg.v13.i30.4141
Assessment of T staging and mesorectal fascia status using high-resolution MRI in rectal cancer with rectal distention
Abstract
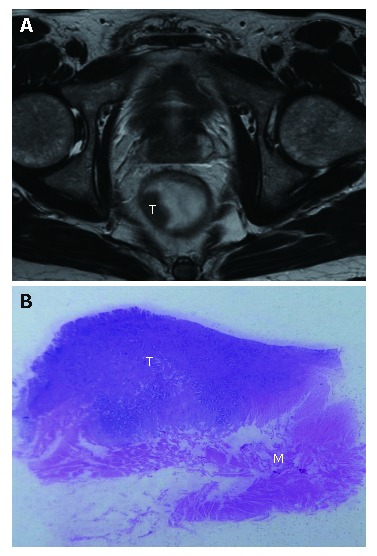
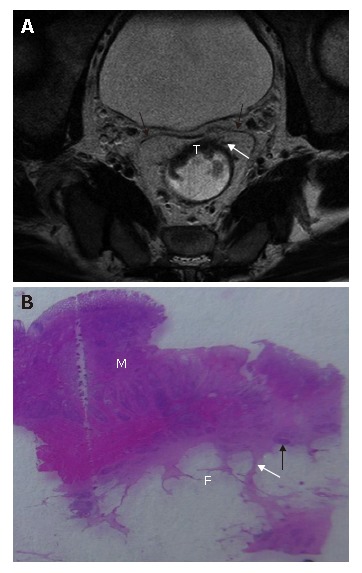
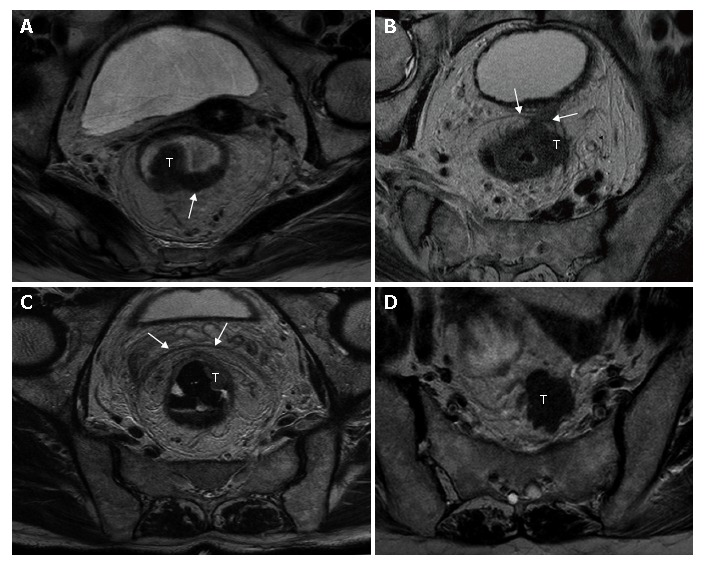
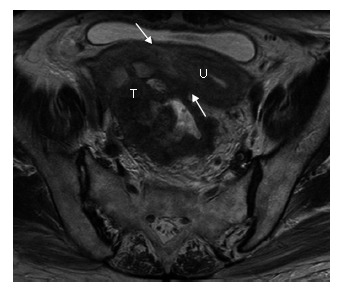
Aim: To determine the accuracy of high-resolution magnetic resonance imaging (MRI) using phased-array coil for preoperative assessment of T staging and mesorectal fascia infiltration in rectal cancer with rectal distention.
Methods: In a prospective study of 67 patients with primary rectal cancer, high-resolution magnetic resonance imaging (in-plane resolution, 0.66 multiply 0.56) with phased-array coil were performed for T-staging and measurement of distance between the tumor and the mesorectal fascia. The assessment of MRI was compared with postoperative histopathologic findings. Sensitivity, specificity, accuracy, positive predictive value, and negative predictive value were evaluated.
Results: The overall magnetic resonance accuracy was 85.1% for T staging and 88% for predicting mesorectal fascia involvement. Magnetic resonance sensitivity, specificity, accuracy, positive predictive value, and negative predictive value was 70%, 97.9%, 89.6%, 93.3% and 88.5% for <or= T2 tumors, 90.5%, 76%, 85.1%, 86.4% and 82.6% for T3 tumors, 100%, 95.2%, 95.5%, 62.5% and 100% for T4 tumors, and 80%, 90.4%, 88%, 70.6% and 94% for predicting mesorectal fascia involvement, respectively.
Conclusion: High-resolution MRI enables accurate preoperative assessment for T staging and mesorectal fascia infiltration in rectal cancer with rectal distention.
Figures

References
-
- Adam IJ, Mohamdee MO, Martin IG, Scott N, Finan PJ, Johnston D, Dixon MF, Quirke P. Role of circumferential margin involvement in the local recurrence of rectal cancer. Lancet. 1994;344:707–711. - PubMed
-
- Nagtegaal ID, Marijnen CA, Kranenbarg EK, van de Velde CJ, van Krieken JH. Circumferential margin involvement is still an important predictor of local recurrence in rectal carcinoma: not one millimeter but two millimeters is the limit. Am J Surg Pathol. 2002;26:350–357. - PubMed
-
- Compton CC, Greene FL. The staging of colorectal cancer: 2004 and beyond. CA Cancer J Clin. 2004;54:295–308. - PubMed
-
- Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet. 1986;1:1479–1482. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
