

Expansion of regulatory T cells in patients with Langerhans cell histiocytosis
- PMID: 17696642
- PMCID: PMC1945037
- DOI: 10.1371/journal.pmed.0040253
Expansion of regulatory T cells in patients with Langerhans cell histiocytosis
Abstract
Background: Langerhans cell histiocytosis (LCH) is a rare clonal granulomatous disease that affects mainly children. LCH can involve various tissues such as bone, skin, lung, bone marrow, lymph nodes, and the central nervous system, and is frequently responsible for functional sequelae. The pathophysiology of LCH is unclear, but the uncontrolled proliferation of Langerhans cells (LCs) is believed to be the primary event in the formation of granulomas. The present study was designed to further investigate the nature of proliferating cells and the immune mechanisms involved in the LCH granulomas.
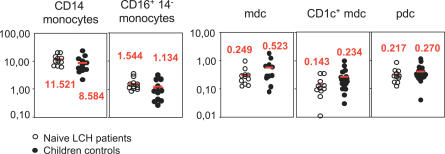
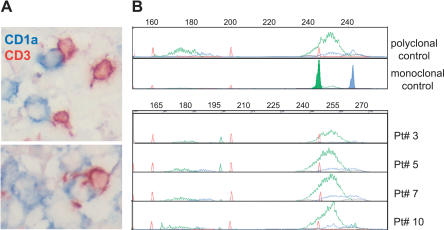
Methods and findings: Biopsies (n = 24) and/or blood samples (n = 25) from 40 patients aged 0.25 to 13 y (mean 7.8 y), were studied to identify cells that proliferate in blood and granulomas. We found that the proliferating index of LCs was low ( approximately 1.9%), and we did not observe expansion of a monocyte or dendritic cell compartment in patients. We found that LCH lesions were a site of active inflammation, tissue remodeling, and neo-angiogenesis, and the majority of proliferating cells were endothelial cells, fibroblasts, and polyclonal T lymphocytes. Within granulomas, interleukin 10 was abundant, LCs expressed the TNF receptor family member RANK, and CD4(+) CD25(high) FoxP3(high) regulatory T cells (T-regs) represented 20% of T cells, and were found in close contact with LCs. FoxP3(+) T-regs were also expanded compared to controls, in the blood of LCH patients with active disease, among whom seven out of seven tested exhibited an impaired skin delayed-type hypersensitivity response. In contrast, the number of blood T-regs were normal after remission of LCH.
Conclusions: These findings indicate that LC accumulation in LCH results from survival rather than uncontrolled proliferation, and is associated with the expansion of T-regs. These data suggest that LCs may be involved in the expansion of T-regs in vivo, resulting in the failure of the host immune system to eliminate LCH cells. Thus T-regs could be a therapeutic target in LCH.
Conflict of interest statement
Figures



References
-
- Lichtenstein L. Histiocytosis X: Integration of eosinophilic granuloma of bone, Letterer-Siwe disease, and Schuller-Christian disease as related manifestations of a single nosologic entity. AMA Arch Pathol. 1953;56:84–102. - PubMed
-
- Favara BE, Steele A. Langerhans cell histiocytosis of lymph nodes: A morphological assessment of 43 biopsies. Pediatr Pathol Lab Med. 1997;17:769–787. - PubMed
-
- Geissmann F, Thomas C, Emile JF, Micheau M, Canioni D, et al. Digestive tract involvement in Langerhans cell histiocytosis. The French Langerhans Cell Histiocytosis Study Group. J Pediatr. 1996;129:836–845. - PubMed
-
- Geissmann F, Lepelletier Y, Fraitag S, Valladeau J, Bodemer C, et al. Differentiation of Langerhans cells in Langerhans cell histiocytosis. Blood. 2001;97:1241–1248. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
