

Mechanisms, molecular and sero-epidemiology of antimicrobial resistance in bacterial respiratory pathogens isolated from Japanese children
- PMID: 17697316
- PMCID: PMC2020463
- DOI: 10.1186/1476-0711-6-7
Mechanisms, molecular and sero-epidemiology of antimicrobial resistance in bacterial respiratory pathogens isolated from Japanese children
Abstract
Background: The clinical management of community-acquired respiratory tract infections (RTIs) is complicated by the increasing worldwide prevalence of antibacterial resistance, in particular, beta-lactam and macrolide resistance, among the most common causative bacterial pathogens. This study aimed to determine the mechanisms and molecular- and sero-epidemiology of antibacterial resistance among the key paediatric respiratory pathogens in Japan.
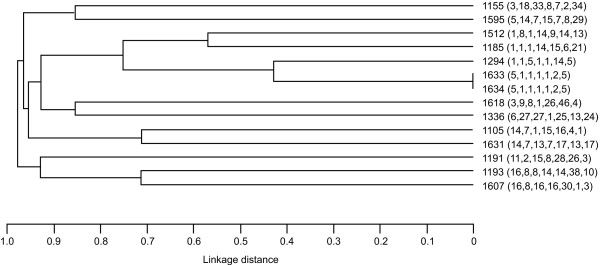
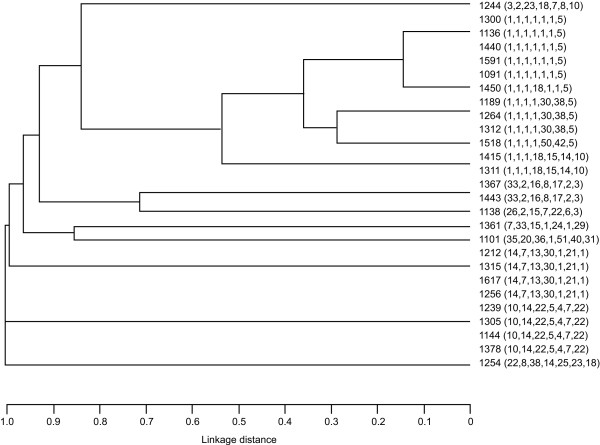
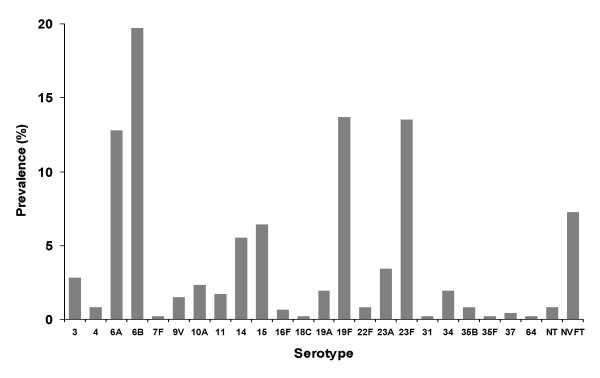
Methods: Isolates were collected at 18 centres in Japan during 2002 and 2003 from children with RTIs as part of the PROTEKT surveillance programme. A proportion of Haemophilus influenzae isolates was subjected to sequencing analysis of the ftsI gene; phylogenetic relatedness was assessed using multilocus sequence typing. Streptococcus pneumoniae isolates were screened for macrolide-resistance genotype by polymerase chain reaction and serotyped using the capsular swelling method. Susceptibility of isolates to selected antibacterials was performed using CLSI methodology.
Results and discussion: Of the 557 H. influenzae isolates collected, 30 (5.4%) were beta-lactamase-positive [BL+], 115 (20.6%) were BL-nonproducing ampicillin-resistant (BLNAR; MIC >or= 4 mg/L) and 79 (14.2%) were BL-nonproducing ampicillin-intermediate (BLNAI; MIC 2 mg/L). Dabernat Group III penicillin binding protein 3 (PBP3) amino acid substitutions in the ftsI gene were closely correlated with BLNAR status but phylogenetic analysis indicated marked clonal diversity. PBP mutations were also found among BL+ and BL-nonproducing ampicillin-sensitive isolates. Of the antibacterials tested, azithromycin and telithromycin were the most active against H. influenzae (100% and 99.3% susceptibility, respectively). A large proportion (75.2%) of the 468 S. pneumoniae isolates exhibited macrolide resistance (erythromycin MIC >or= 1 mg/L); erm(B) was the most common macrolide resistance genotype (58.8%), followed by mef(A) (37.2%). The most common pneumococcal serotypes were 6B (19.7%), 19F (13.7%), 23F (13.5%) and 6A (12.8%). Telithromycin and amoxicillin-clavulanate were the most active antibacterials against S. pneumoniae (99.8% and 99.6% susceptibility, respectively).
Conclusion: Approximately one-third of H. influenzae isolates from paediatric patients in Japan are BLNAI/BLNAR, mainly as a result of clonally diverse PBP3 mutations. Together with the continued high prevalence of pneumococcal macrolide resistance, these results may have implications for the clinical management of paediatric RTIs in Japan.
Figures
Similar articles
-
Serotypes, antimicrobial susceptibility, and beta-lactam resistance mechanisms of clinical Haemophilus influenzae isolates from Bulgaria in a pre-vaccination period.Scand J Infect Dis. 2013 Feb;45(2):81-7. doi: 10.3109/00365548.2012.710854. Epub 2012 Sep 19. Scand J Infect Dis. 2013. PMID: 22992181
-
Antimicrobial resistance in Haemophilus influenzae isolated from the nasopharynx among Japanese children with acute otitis media.Acta Otolaryngol. 2006 Feb;126(2):130-7. doi: 10.1080/00016480500312455. Acta Otolaryngol. 2006. PMID: 16428188
-
Mutant ftsI genes in the emergence of penicillin-binding protein-mediated beta-lactam resistance in Haemophilus influenzae in Norway.Clin Microbiol Infect. 2010 Aug;16(8):1117-24. doi: 10.1111/j.1469-0691.2009.03052.x. Epub 2009 Sep 8. Clin Microbiol Infect. 2010. PMID: 19737286
-
Antibiotic non-susceptibility among Streptococcus pneumoniae and Haemophilus influenzae isolates identified in African cohorts: a meta-analysis of three decades of published studies.Int J Antimicrob Agents. 2013 Dec;42(6):482-91. doi: 10.1016/j.ijantimicag.2013.08.012. Epub 2013 Sep 23. Int J Antimicrob Agents. 2013. PMID: 24139883 Review.
-
[Antimicrobial susceptibility of Streptococcus pneumoniae and Haemophilus influenzae isolated in major hospitals in Nagano Prefecture].Jpn J Antibiot. 2002 Oct;55(5):524-36. Jpn J Antibiot. 2002. PMID: 12532636 Review. Japanese.
Cited by
-
Multilocus sequence typing and ftsI sequencing: a powerful tool for surveillance of penicillin-binding protein 3-mediated beta-lactam resistance in nontypeable Haemophilus influenzae.BMC Microbiol. 2014 May 20;14:131. doi: 10.1186/1471-2180-14-131. BMC Microbiol. 2014. PMID: 24884375 Free PMC article.
-
Social-economic factors and irrational antibiotic use as reasons for antibiotic resistance of bacteria causing common childhood infections in primary healthcare.Eur J Pediatr. 2012 May;171(5):767-77. doi: 10.1007/s00431-011-1592-5. Epub 2011 Oct 7. Eur J Pediatr. 2012. PMID: 21987082 Review.
References
-
- File TM. The epidemiology of respiratory tract infections. Semin Respir Infect. 2000;15:184–194. - PubMed
-
- Bartlett JG, Breiman RF, Mandell LA, File TM., Jr Community-acquired pneumonia in adults: guidelines for management. Clin Infect Dis. 1998;26:811–838. - PubMed
-
- Felmingham D. Evolving resistance patterns in community-acquired respiratory tract pathogens: first results from the PROTEKT global surveillance study. J Infect. 2002;44:3–10. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
